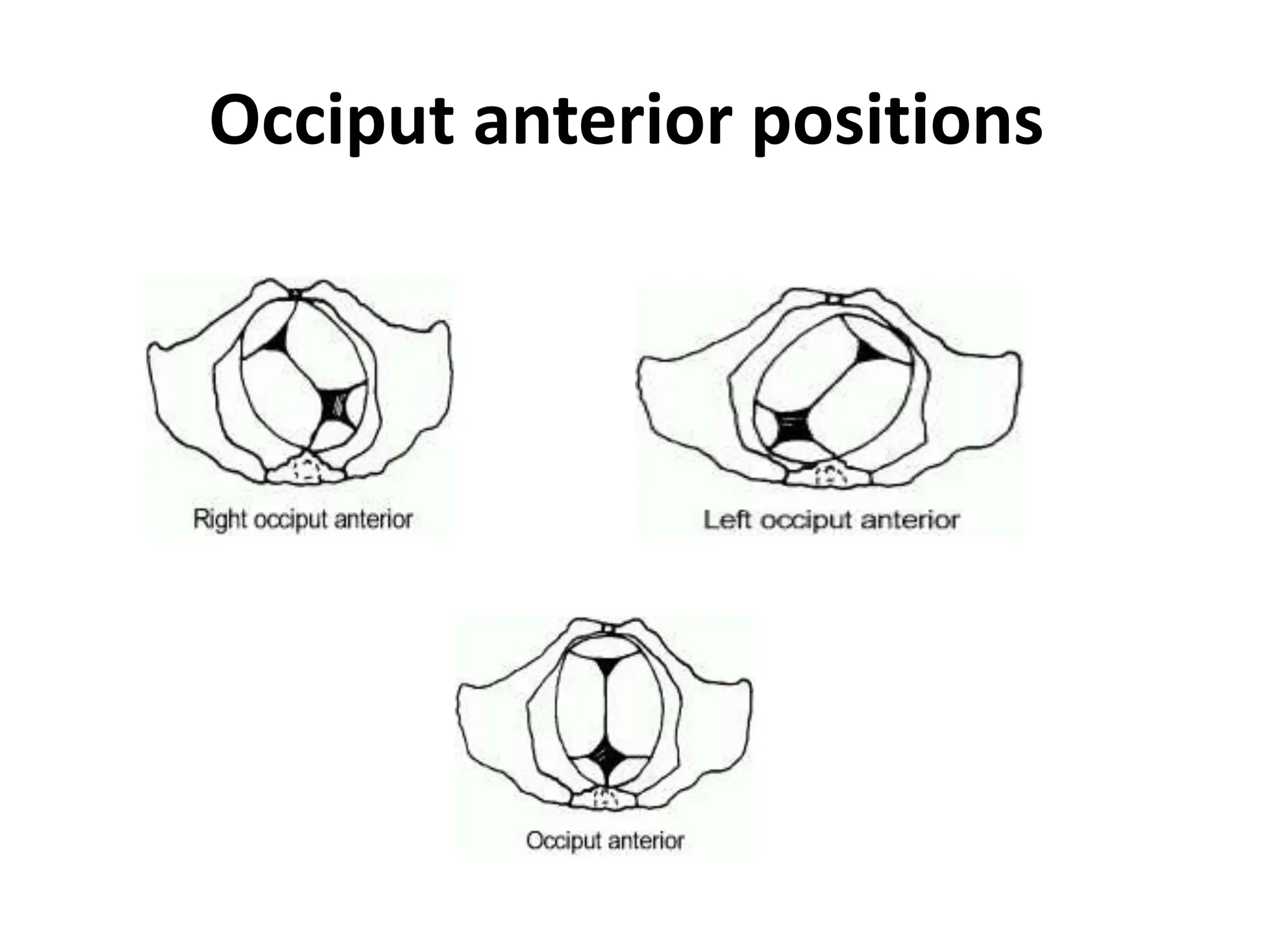
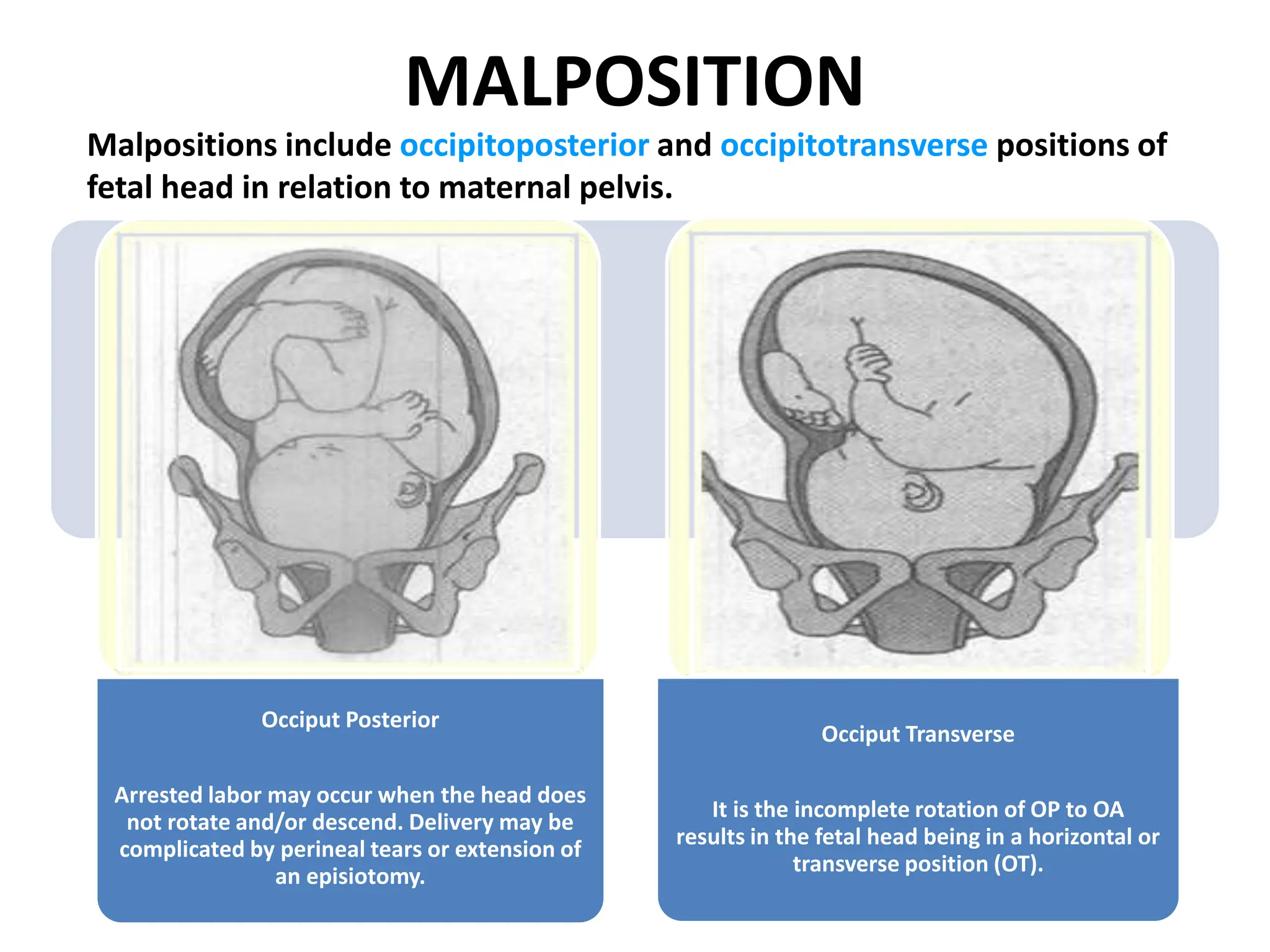
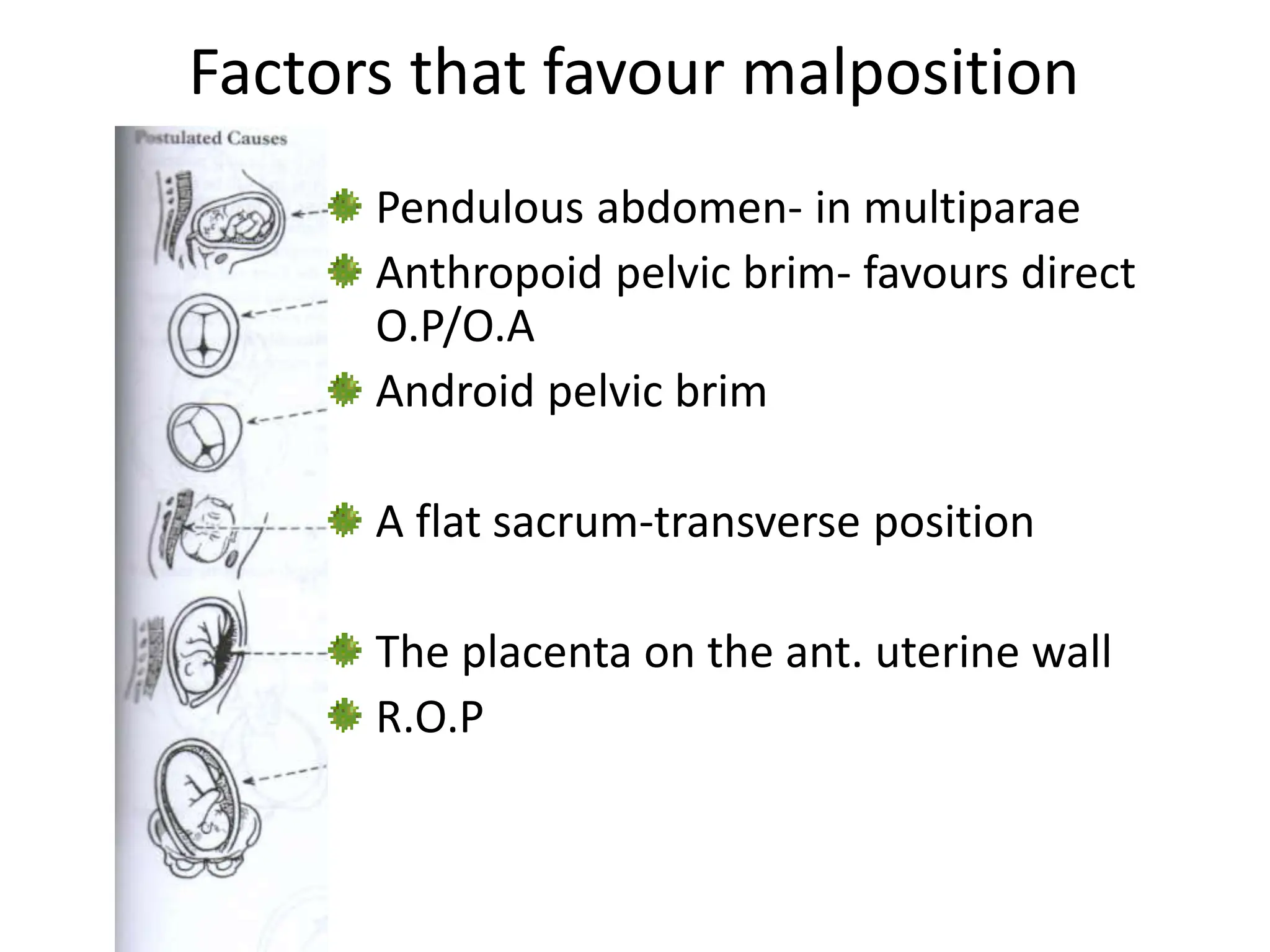
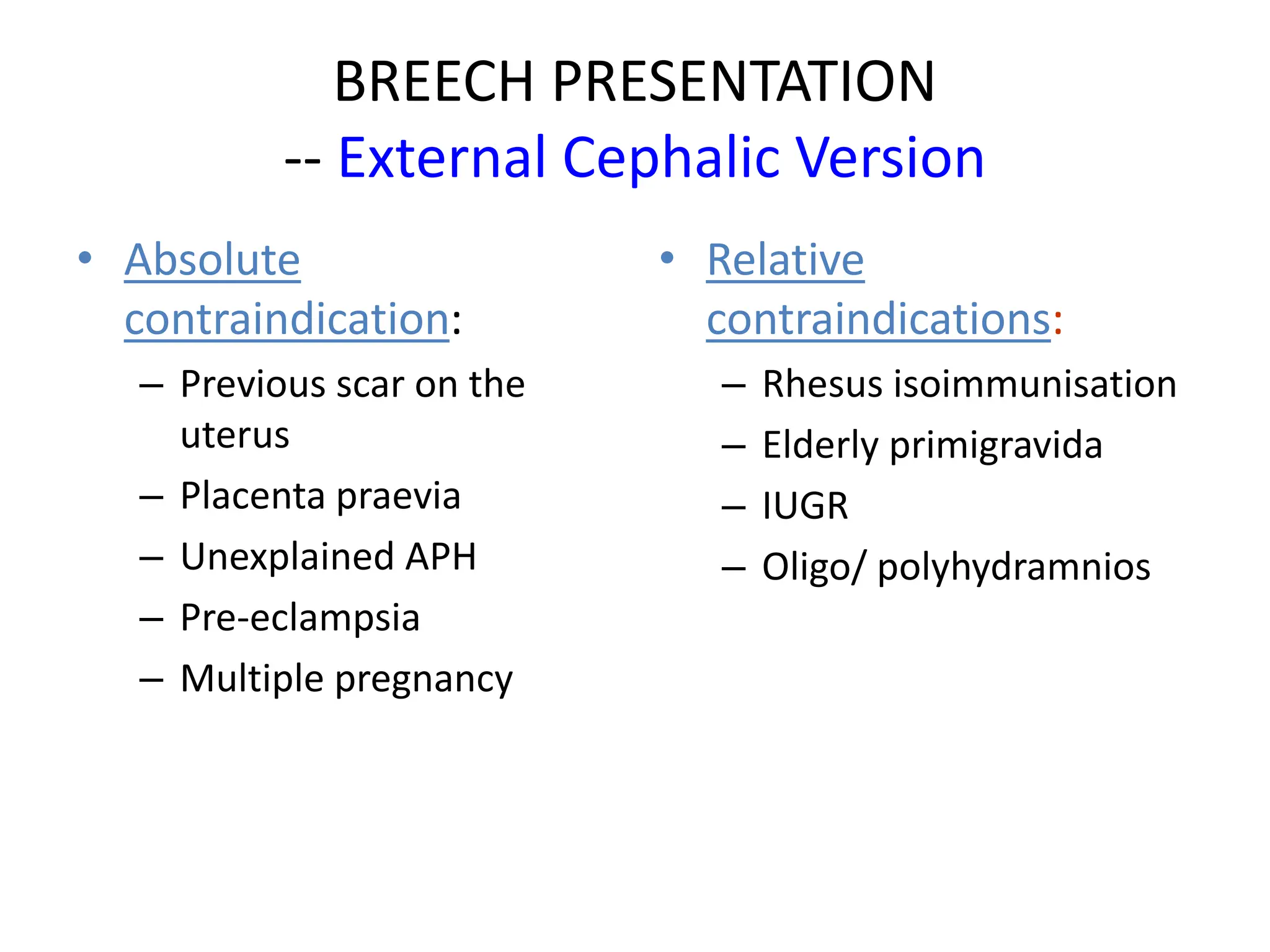
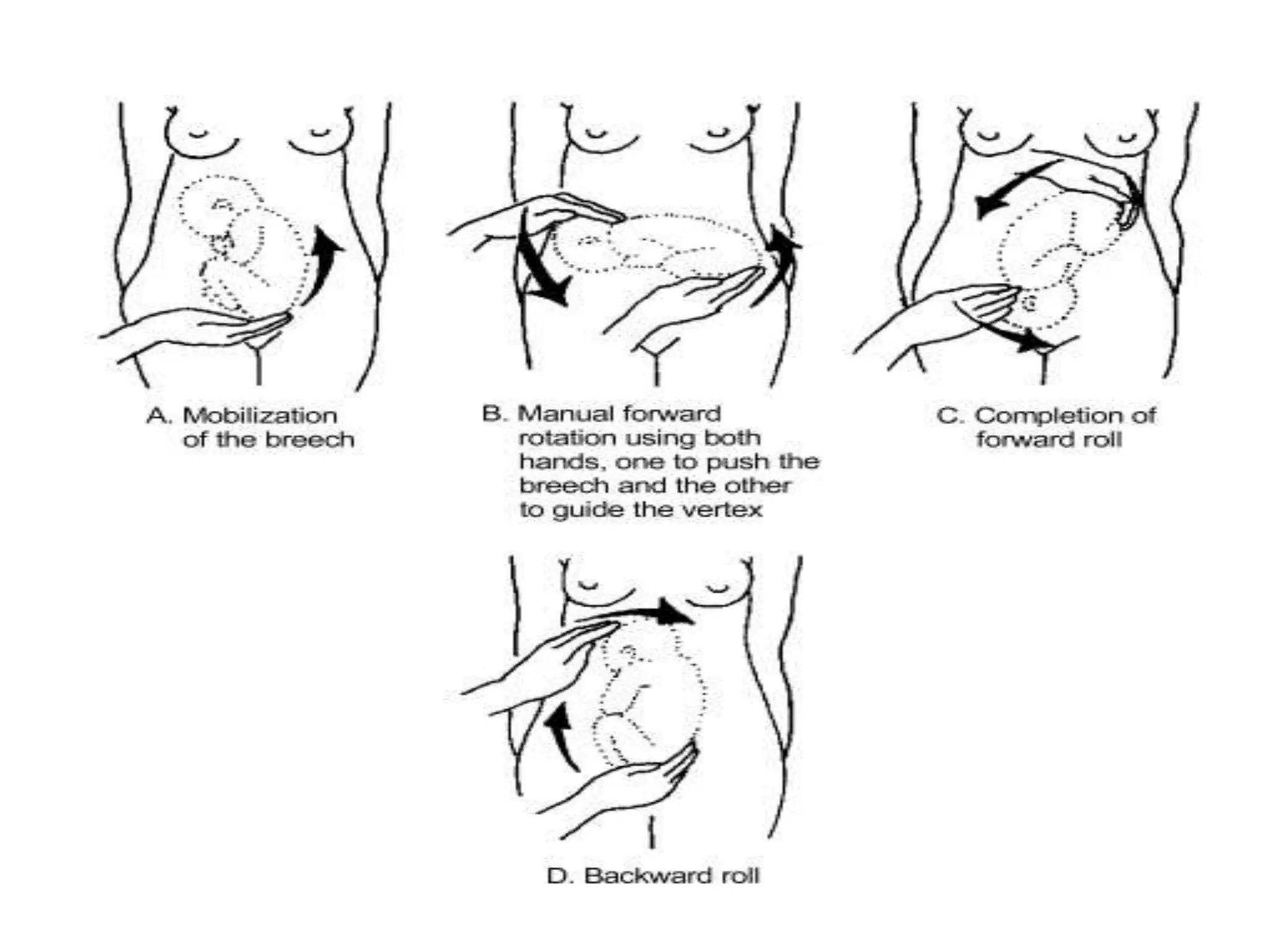
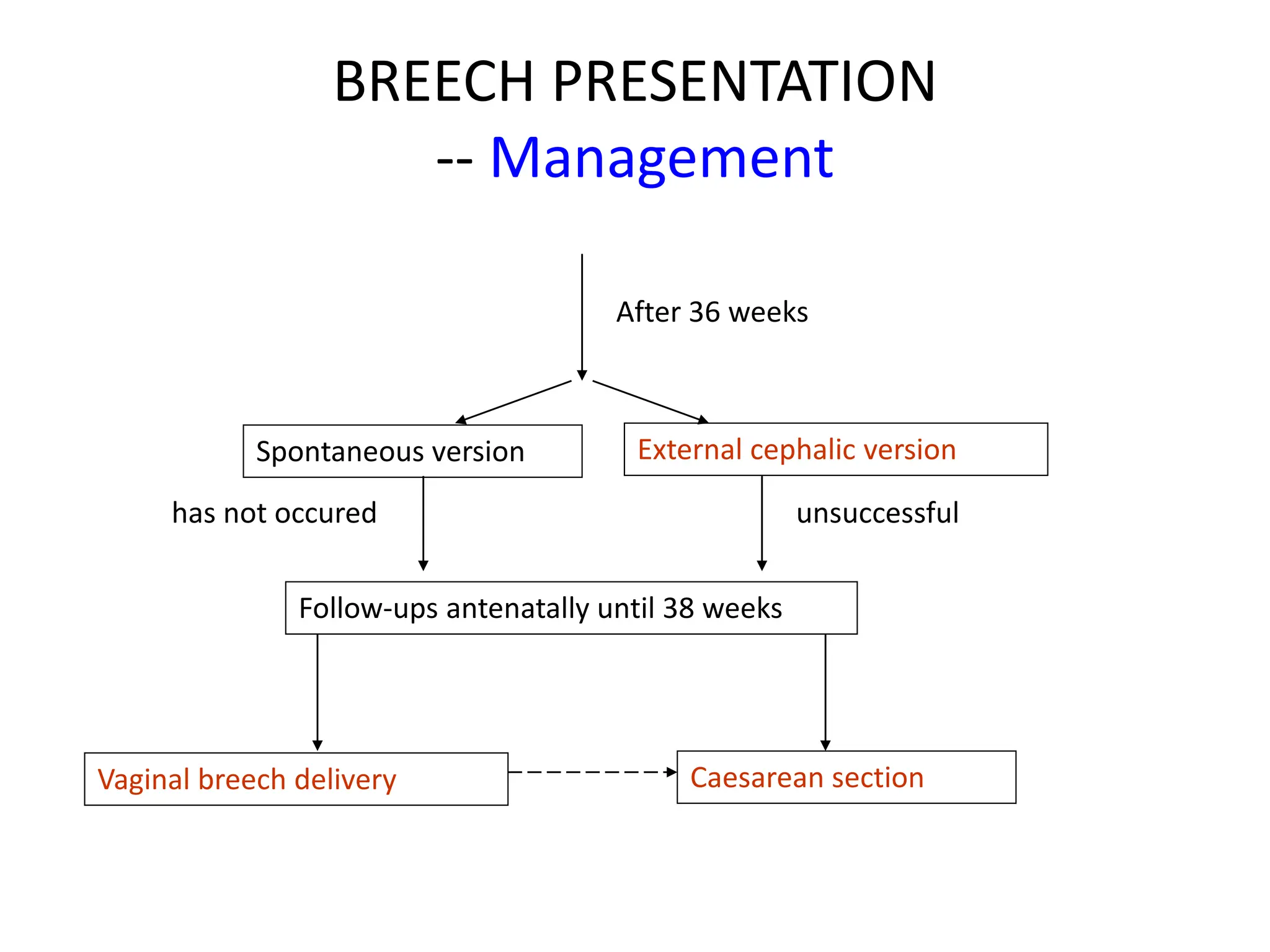
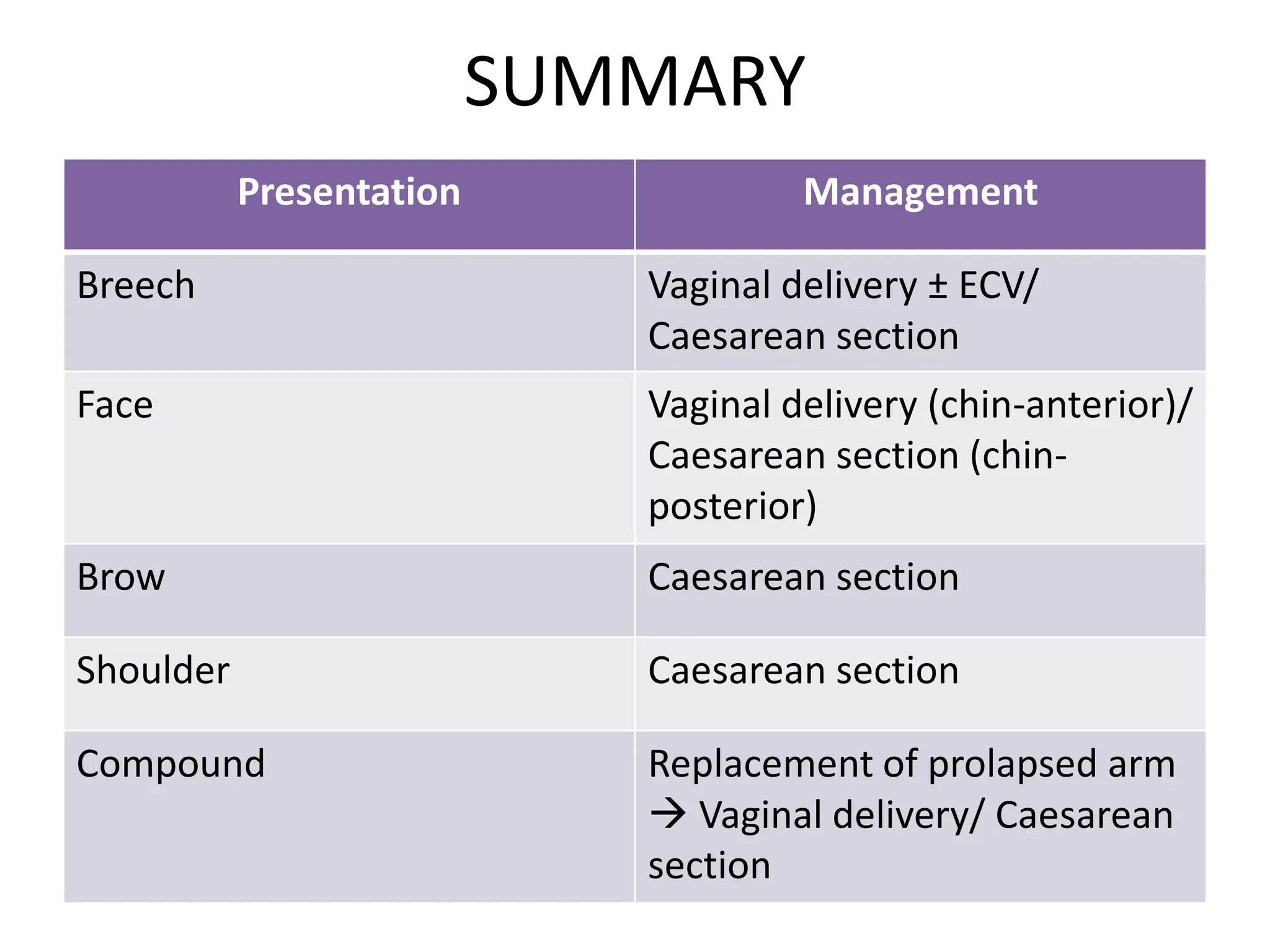
Malpresentation refers to any non-vertex fetal position including breech, brow, transverse, or face, while malposition refers to positions other than occiput anterior. Common malpositions include occiput posterior and occiput transverse, which can complicate delivery and increase risks of tears or difficult extraction. Management may include external cephalic version, breech vaginal delivery if risks are low or caesarean section, especially for breech after 36 weeks given higher safety shown by studies for caesarean in this situation.