Downloaded 32 times
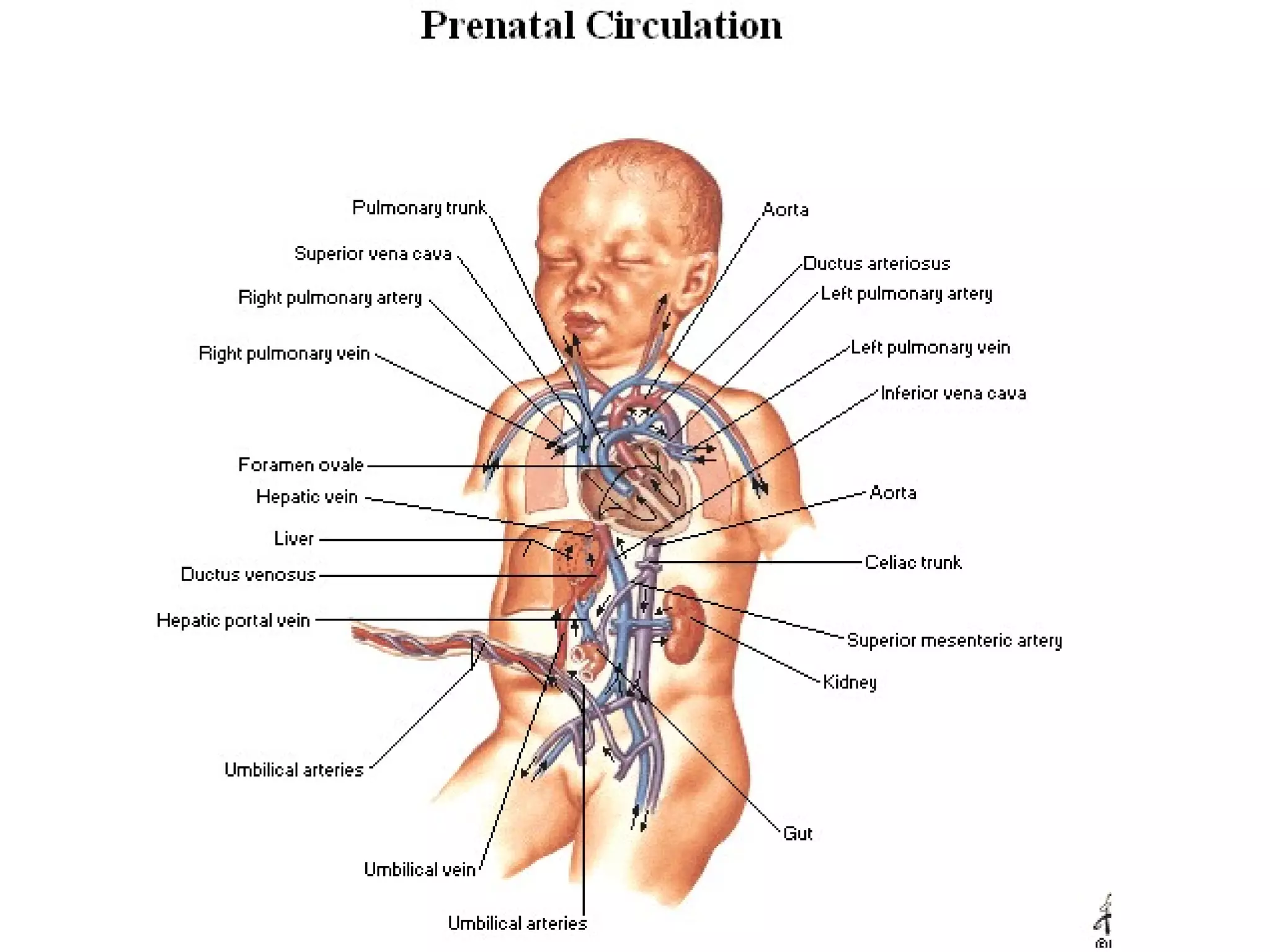
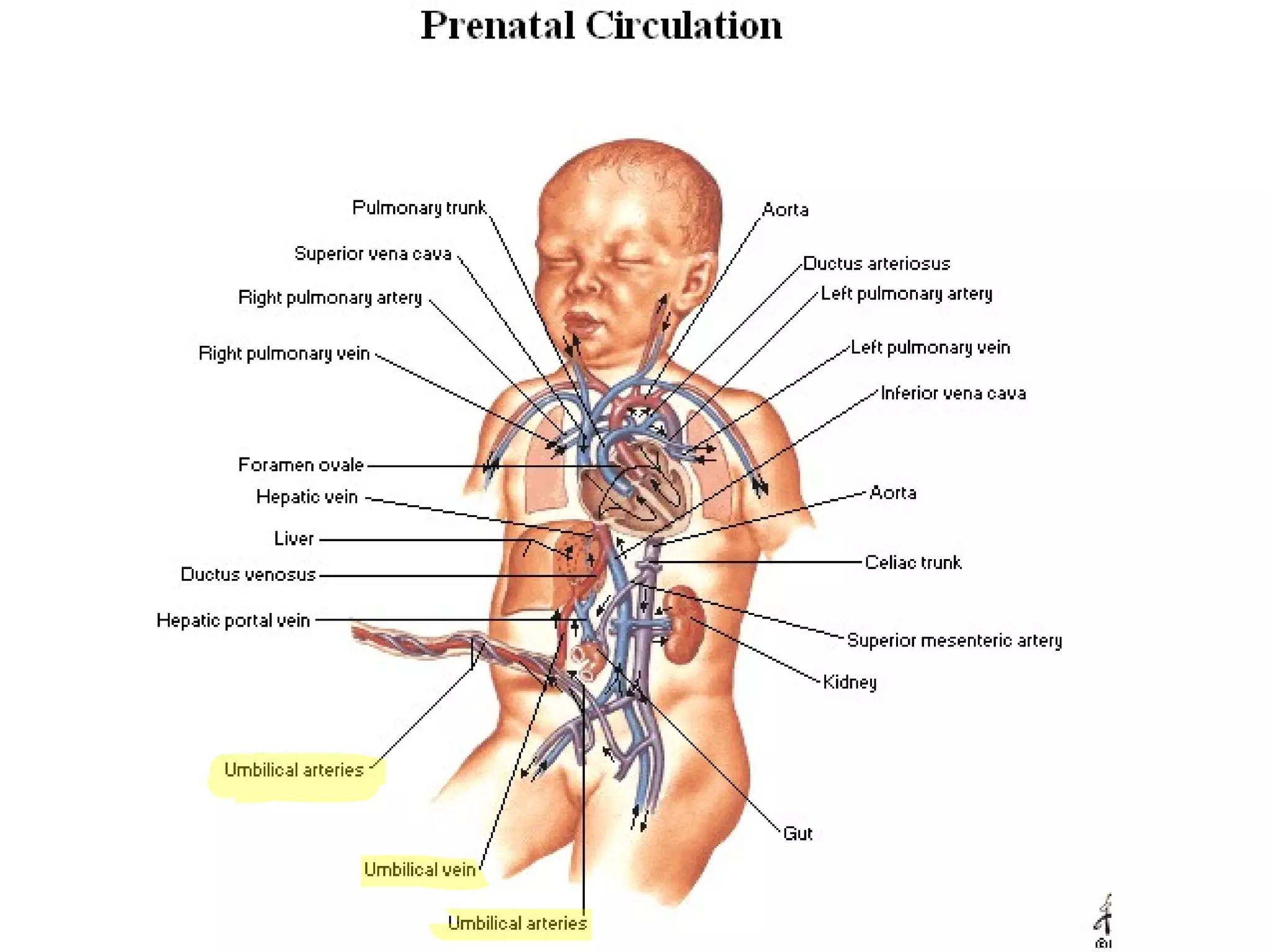
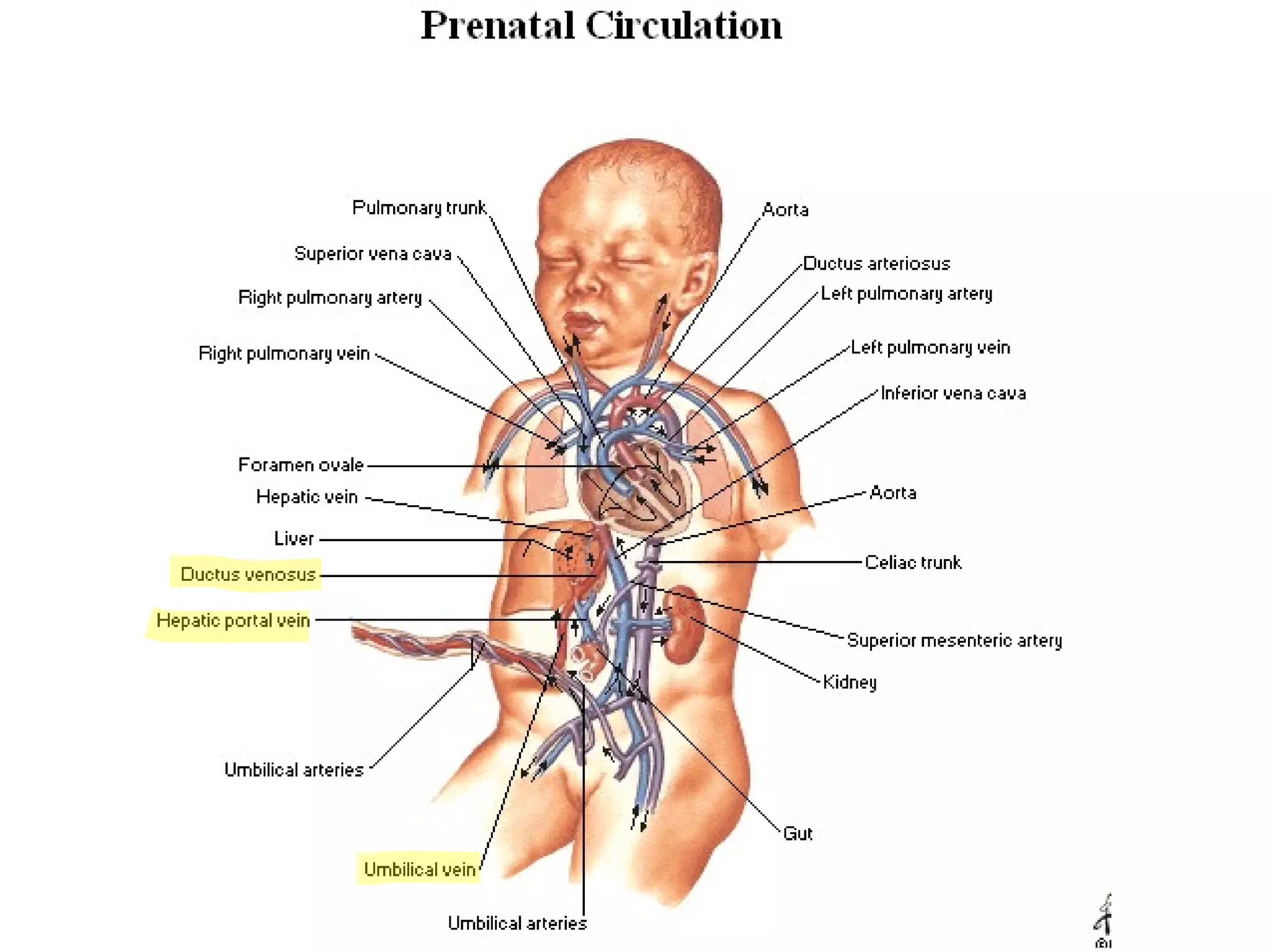
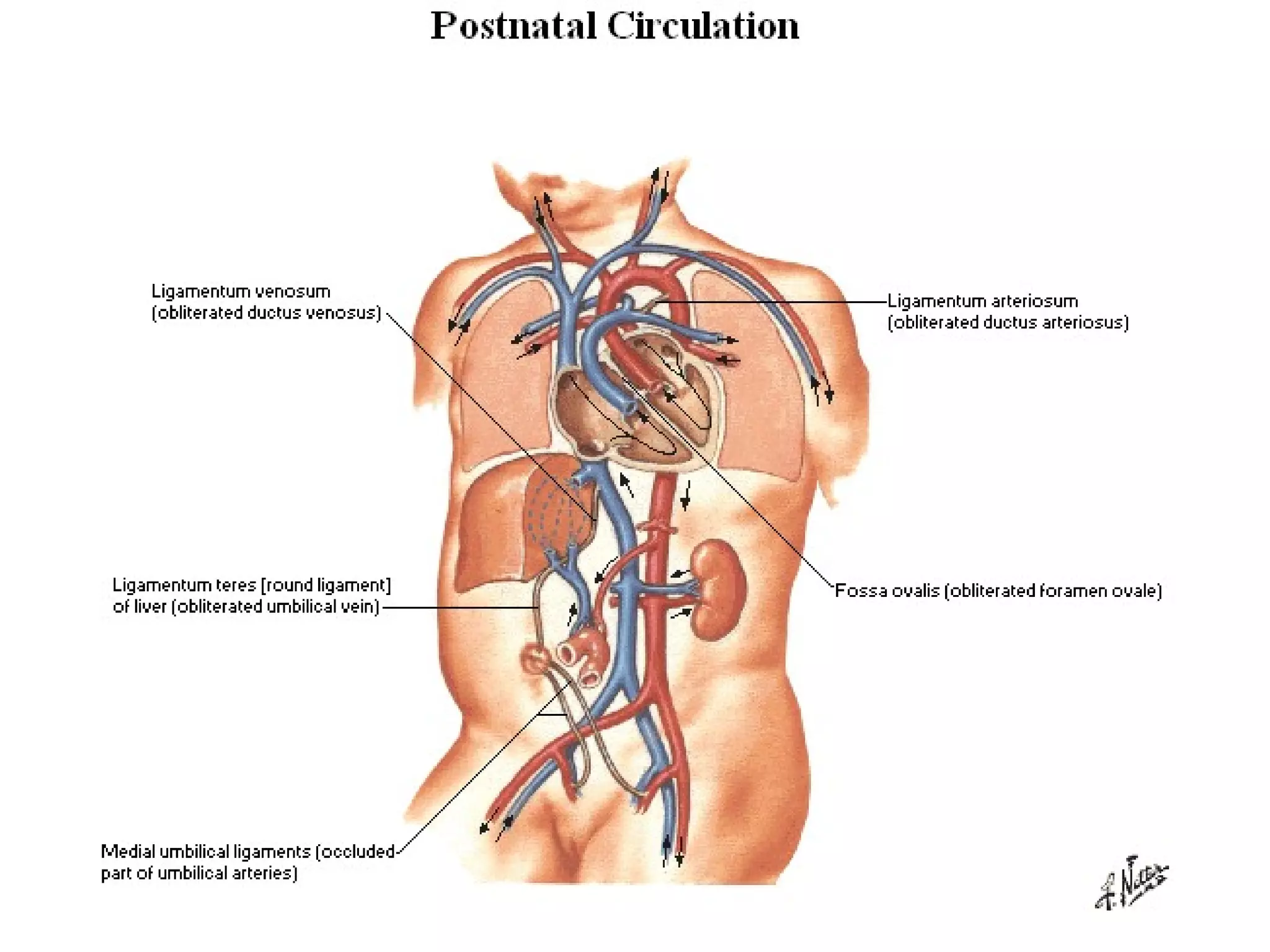
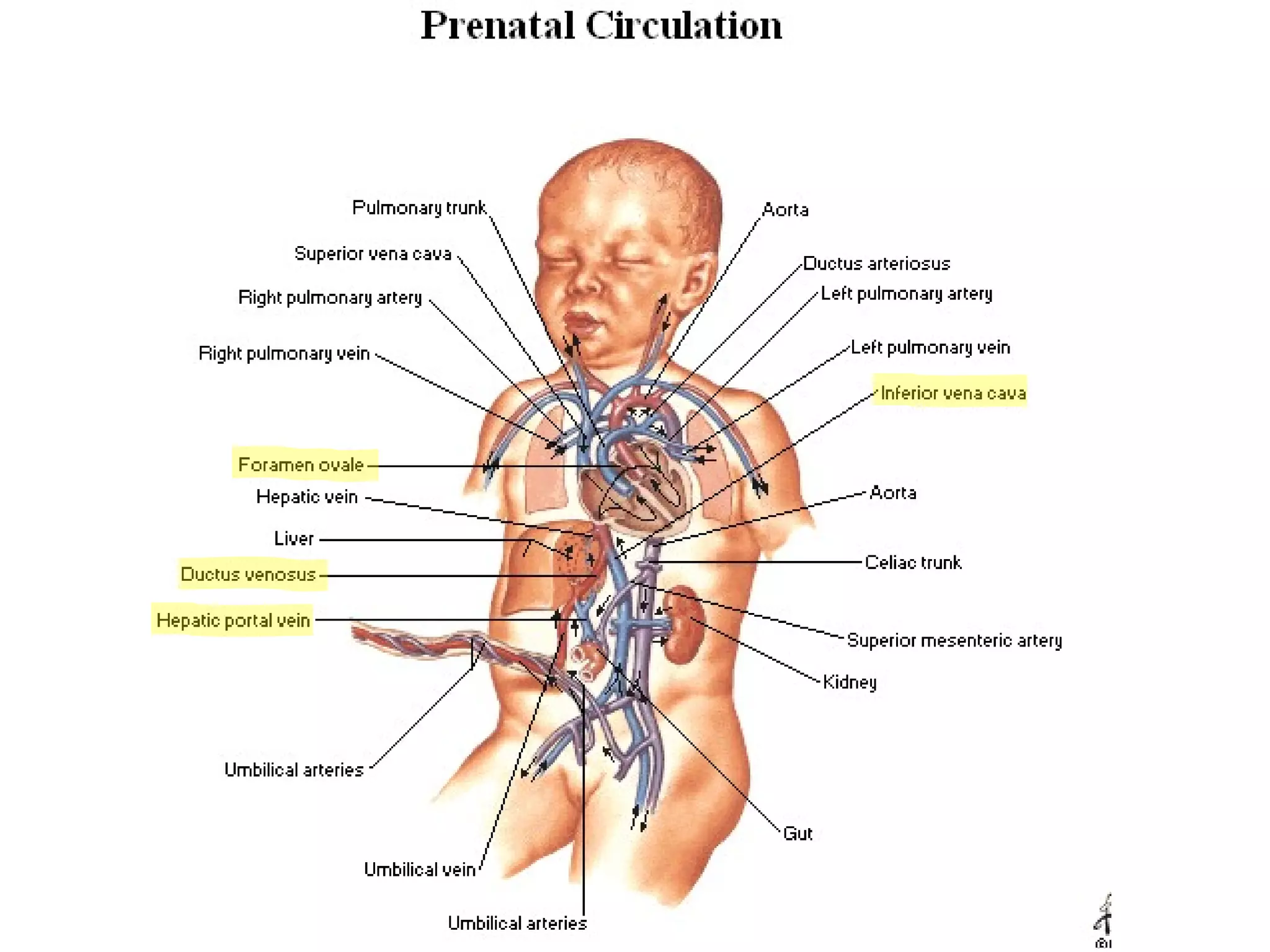
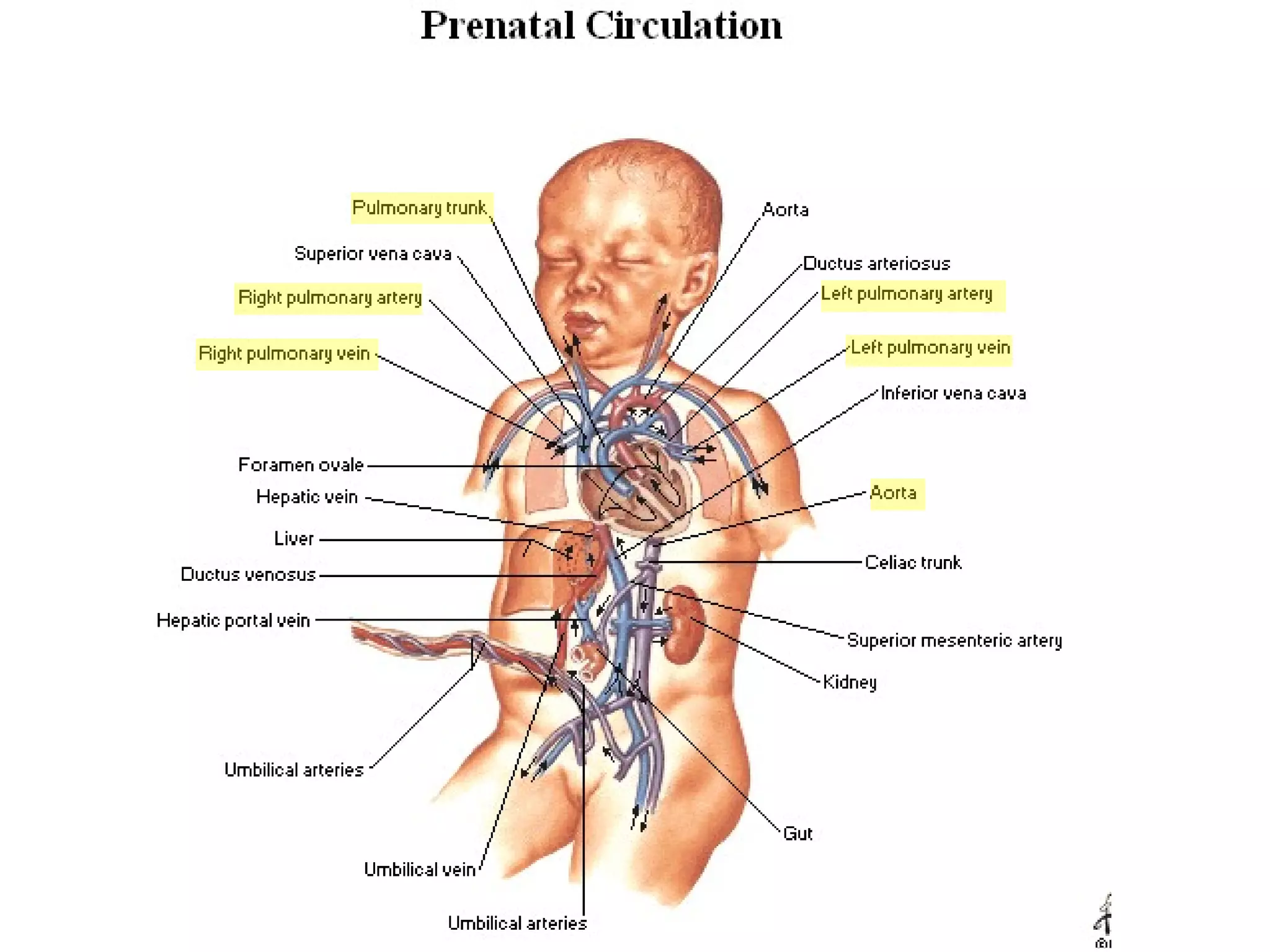
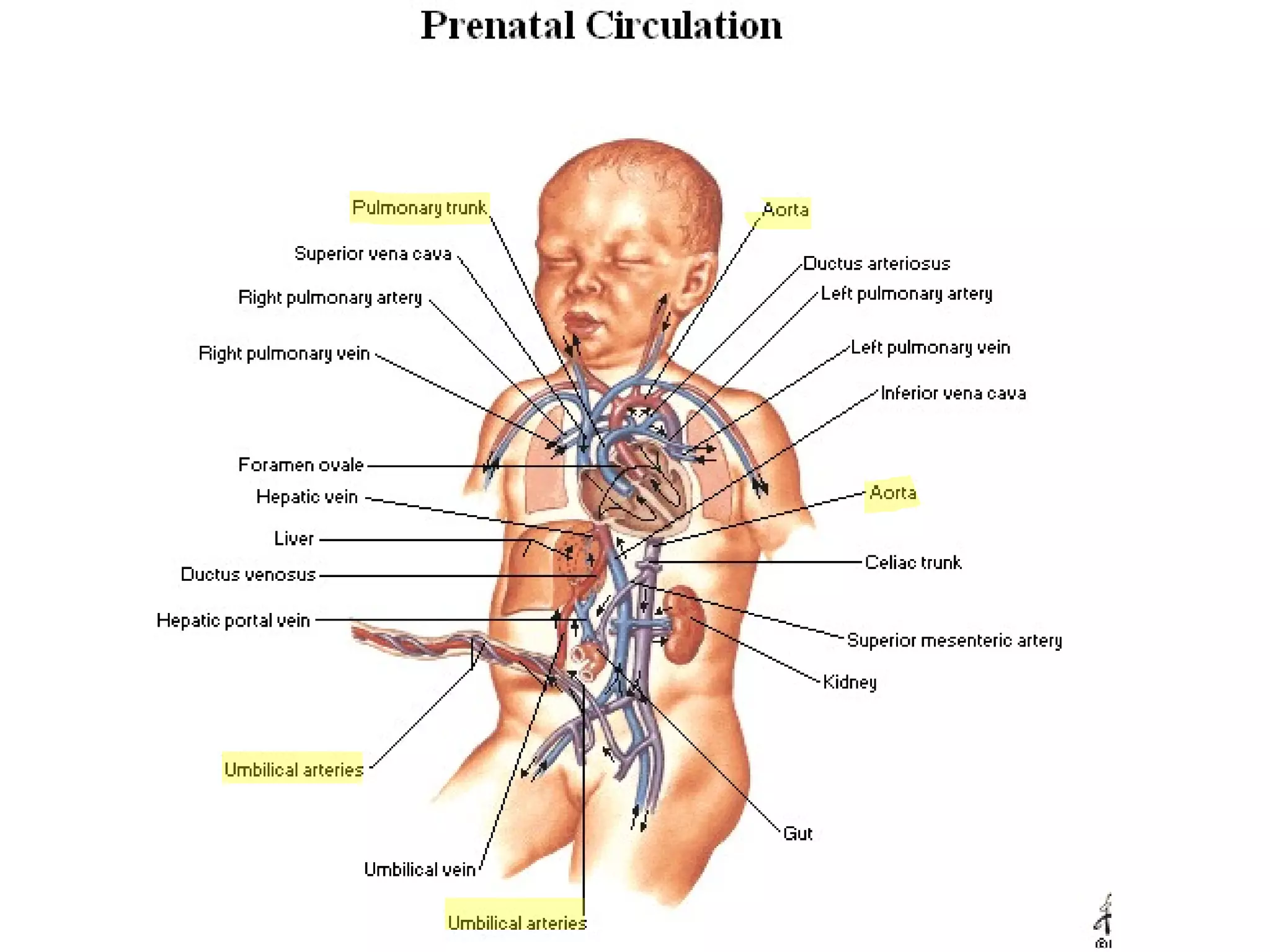
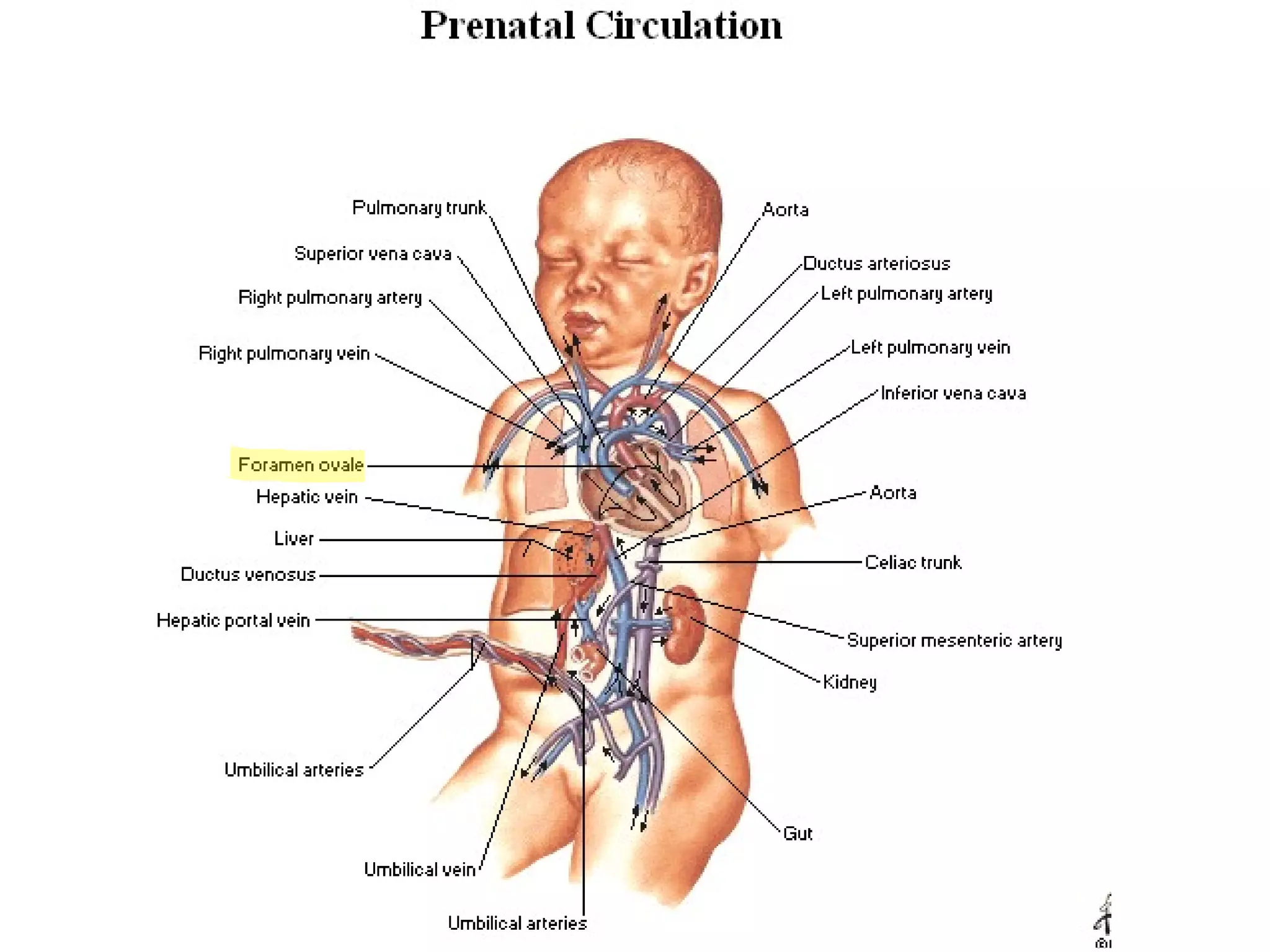
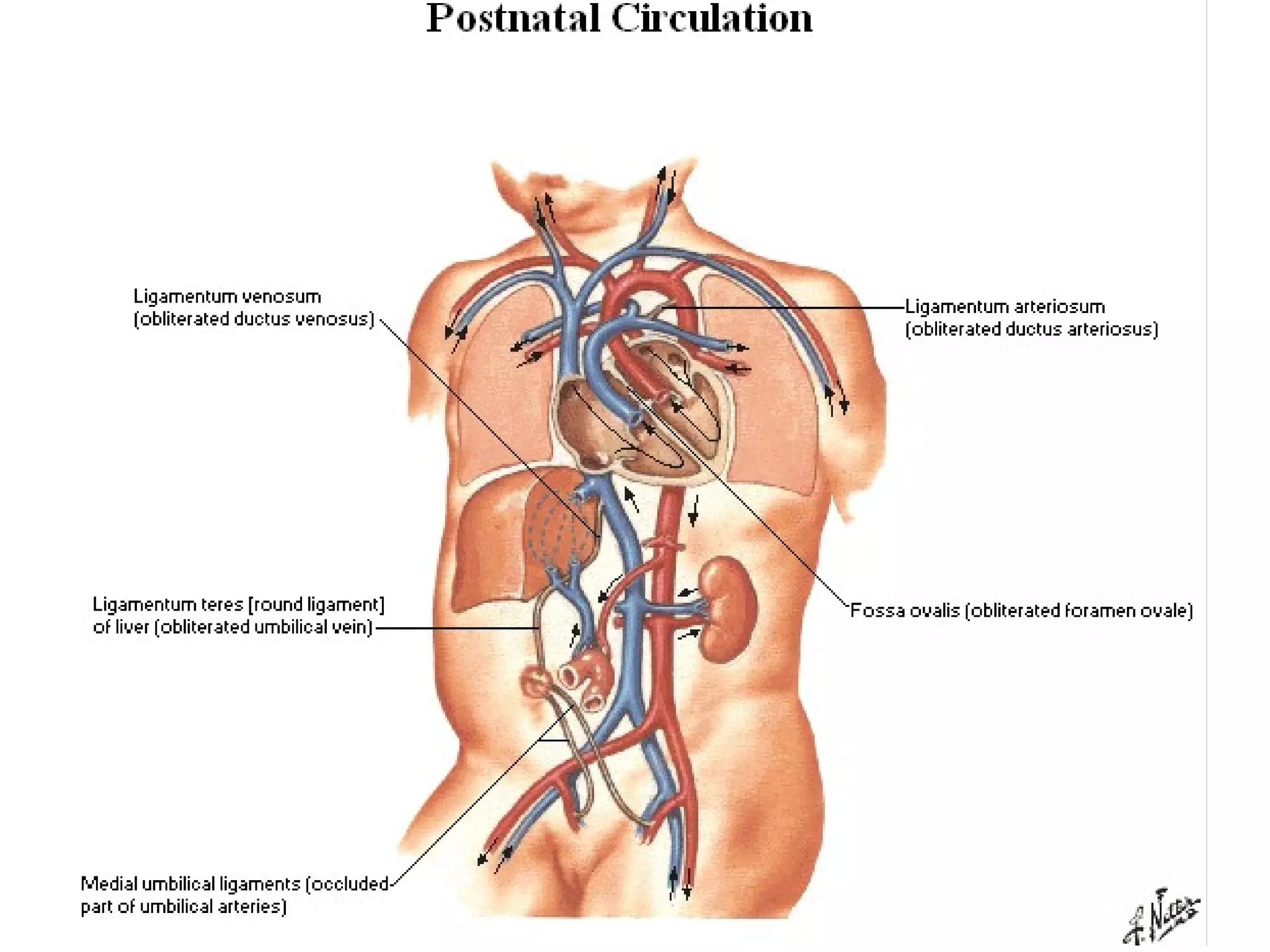
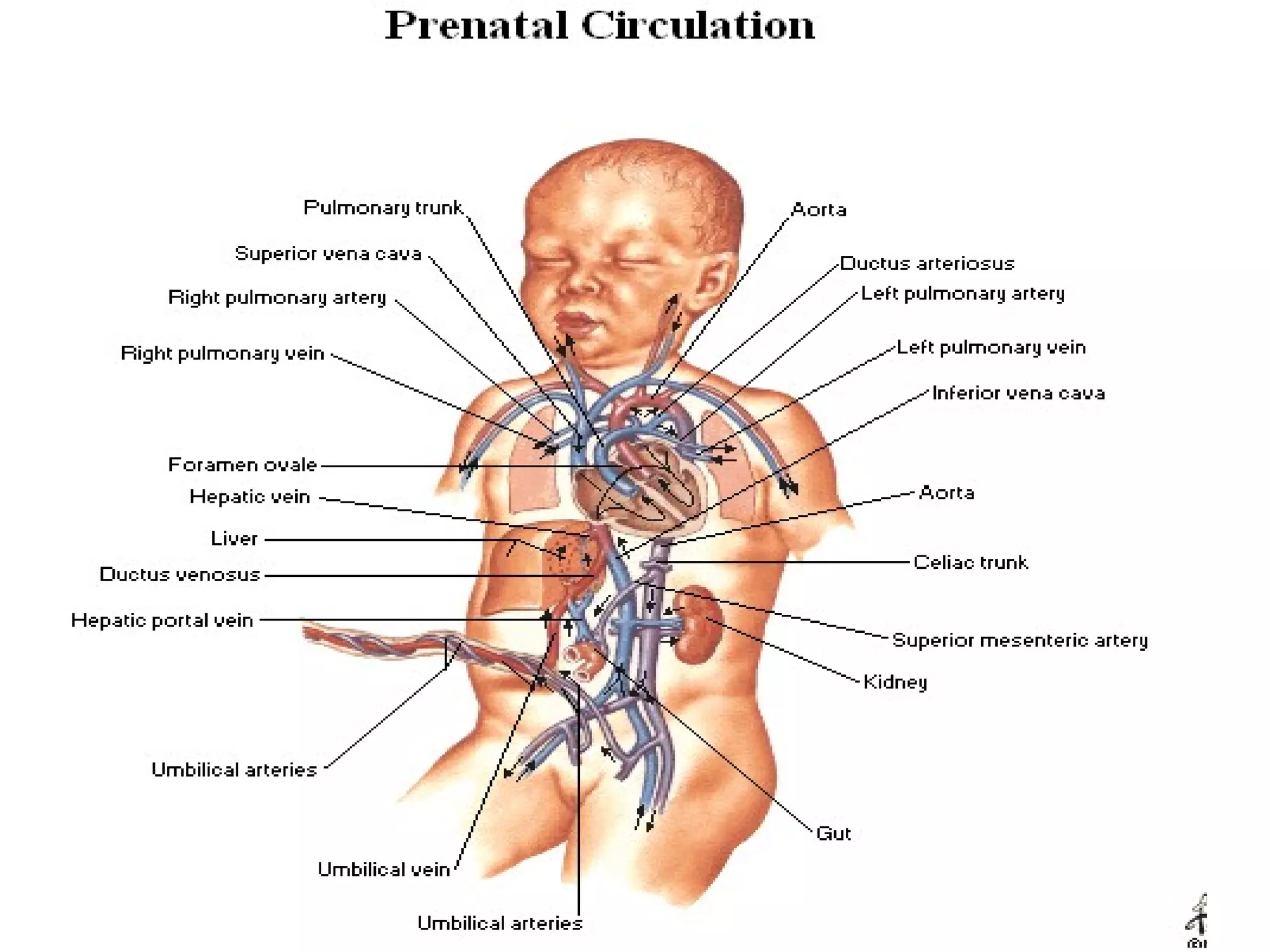
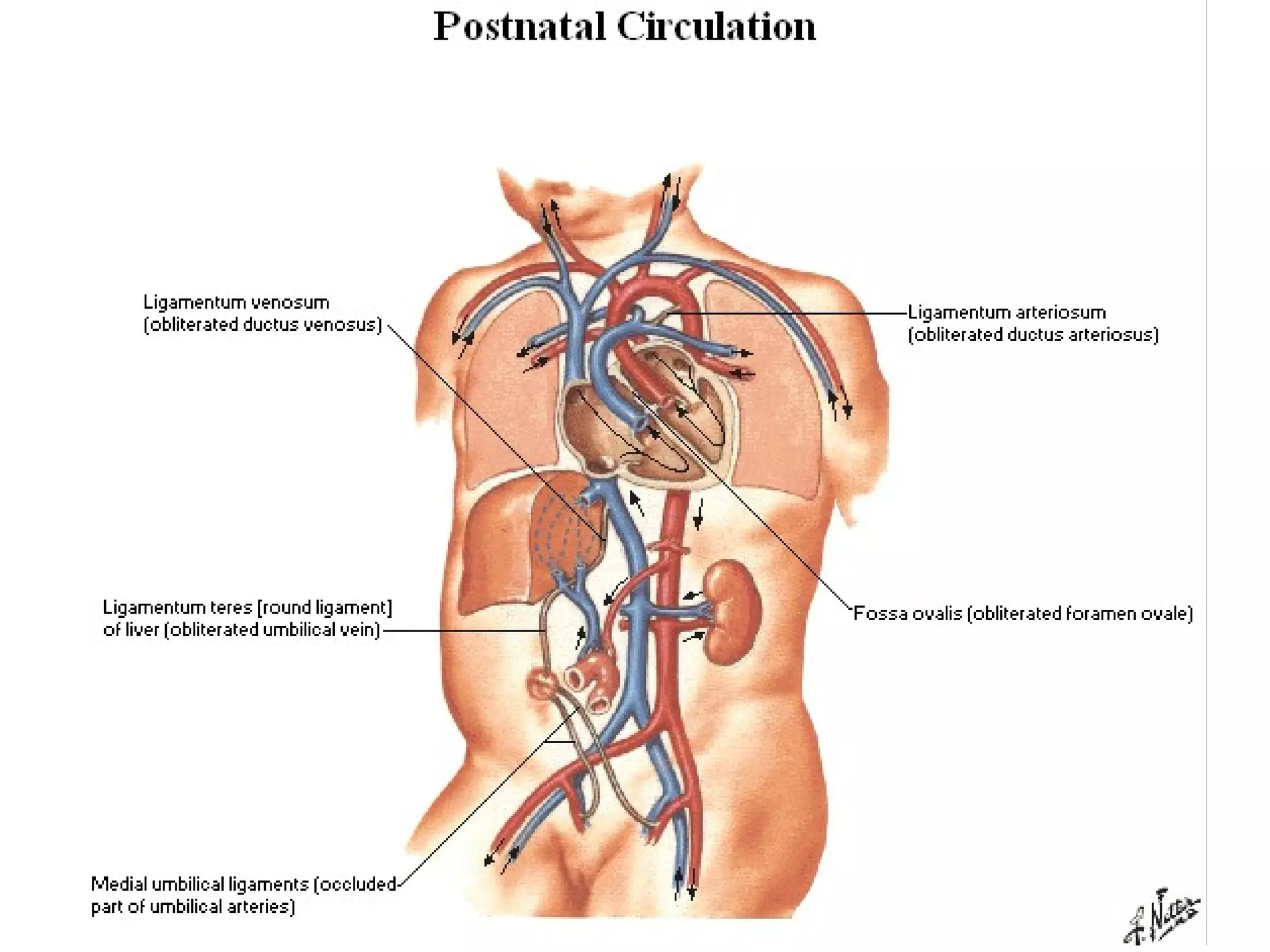


The document summarizes the fetal circulation system and how it differs from the newborn circulation. In the fetus, oxygen-rich blood from the placenta travels through the umbilical vein to the liver and mixes with venous blood before entering the heart. It then passes through the foramen ovale into the left side of the heart and mixes with pulmonary blood to be pumped throughout the body. After birth, the foramen ovale, ductus arteriosus, and umbilical vessels close as the lungs inflate and the placental circulation is lost. This allows the cardiovascular system to transition to adult circulation.








































































































