Download to read offline
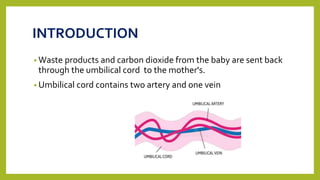
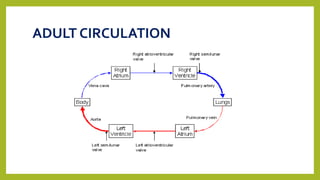
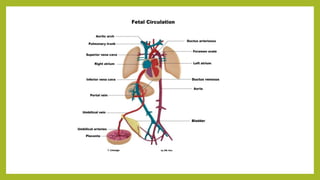
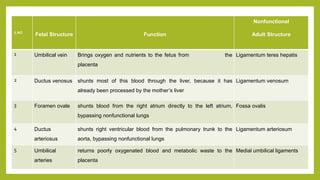
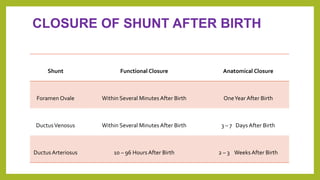
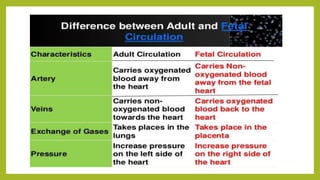


The document summarizes fetal circulation during pregnancy and at birth. During pregnancy, the placenta functions as the lungs and exchanges gases. The umbilical cord connects the fetus to the placenta, carrying oxygenated blood, nutrients to the fetus and deoxygenated blood, waste products back. In the fetus, blood circulation bypasses the nonfunctional lungs and liver through special openings called shunts. At birth, with the first breath the lungs inflate and the ductus arteriosus and foramen ovale close, establishing adult-like circulation.