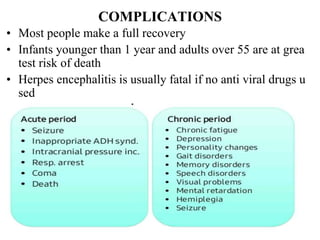
The document presents a seminar on encephalitis, defining it as inflammation of the brain and describing its main types, causes, symptoms, diagnostic tests, treatment including pharmacological and nursing management, complications, and prevention methods. Encephalitis is usually caused by a viral infection but can also be caused by bacteria, and symptoms may include fever, headache, nausea, and confusion.