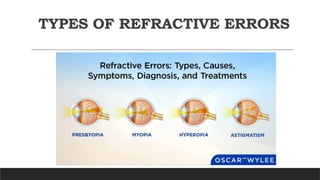
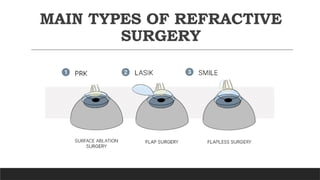
Refractive surgery has revolutionized ophthalmology by offering patients alternatives to spectacles and contact lenses for correction of refractive errors such as myopia, hyperopia, and astigmatism. This presentation provides an overview of the most common surgical techniques—including Photorefractive Keratectomy (PRK), Laser-Assisted In Situ Keratomileusis (LASIK), and Small Incision Lenticule Extraction (SMILE)—highlighting their indications, mechanisms, advantages, and limitations.
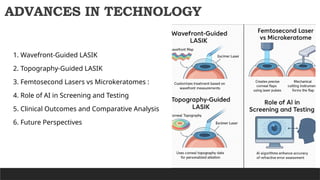
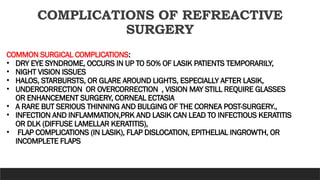
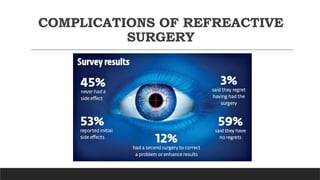
The talk will also explore patient selection criteria, preoperative evaluation, and postoperative care, with emphasis on minimizing complications such as dry eye, corneal ectasia, and visual aberrations. Recent technological advances, including wavefront-guided ablations and femtosecond laser platforms, will be discussed in relation to safety and precision.
By the end of this presentation, attendees will gain a comprehensive understanding of the principles and outcomes of refractive surgery, equipping them to better counsel patients and recognize potential risks and benefit