Downloaded 114 times

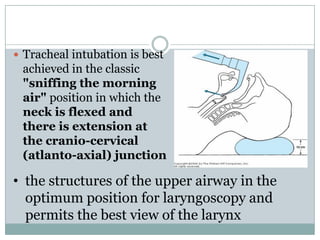

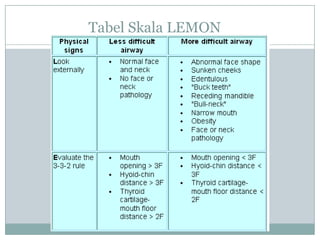
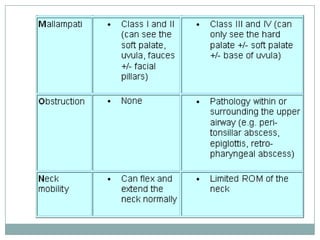
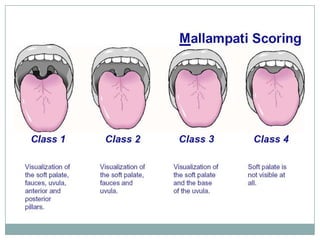
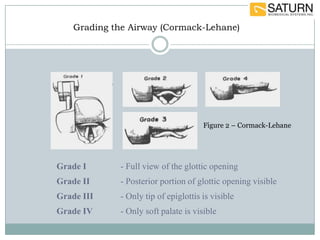
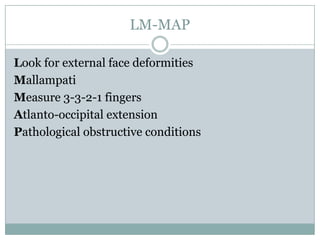
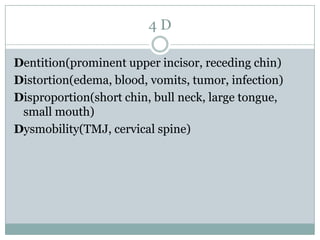
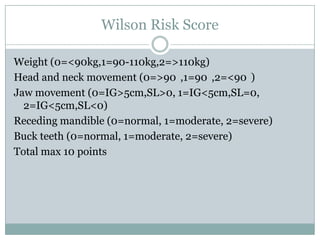
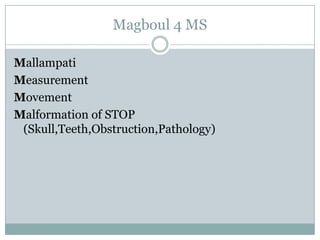
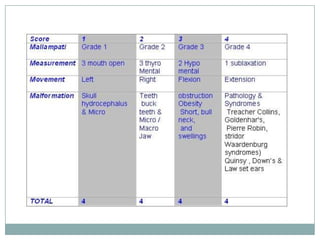
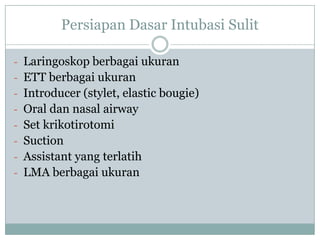

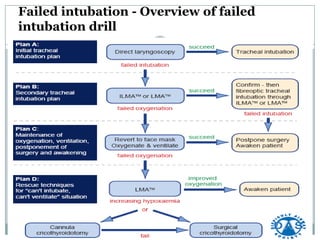
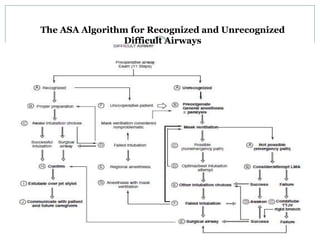
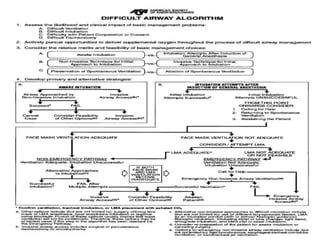

This document discusses difficult intubation and airways. It defines difficult airway as difficulty with facemask ventilation or tracheal intubation. The incidence is estimated between 3-18%. Optimal positioning for intubation is neck flexion with atlanto-axial extension. Several scales are used to evaluate difficulty, including LEMON, LM MAP, 4D, Wilson Risk Scale, and Magboul 4M. Preparations for difficult intubation include different sized laryngoscopes, ET tubes, introducers, airways, and LMAs. Special techniques discussed are awake intubation and awake tracheostomy under local anesthesia. The ASA algorithm provides guidance for recognized and unrecognized difficult airways.























![lapjag_cantik[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lapjagcantik1-230513012817-d8d260b5-thumbnail.jpg?width=640&height=640&fit=bounds)





























![Anesthesia_for_Airway_management_and_Difficult_airway_Algorithmss[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforairwaymanagementanddifficultairwayalgorithmss11-250722203414-f94048f1-thumbnail.jpg?width=640&height=640&fit=bounds)




























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

