Definition
• Difficult airway: a clinical situation where a healthcare provider
who is skilled at airway management encounter difficulties with bag-
mask ventilation, supraglottic airway, laryngoscopy, passage of
ETT through the cords, infraglottic airway or surgical airway.
• Difficult intubation according to (ASA): 'an intubation during
which the insertion of the endotracheal tube takes more than 10
min, and/or requires more than three attempts by an experienced
anesthesiologist'
4.
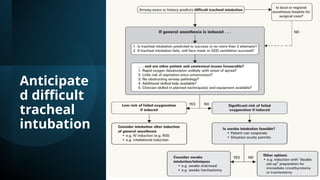
Evaluation of Difficultairway
• pre-operative assessment (history of previous difficult airway, airway
examination) and preoxygenation are important preventative measures.
• LEMON
look - (obesity, beard, dental/facial abnormalities, neck, facial/neck trauma)
Evaluate 3-2-1 rule
Mallampati score
Obstruction – stridor, foreign bodies
Neck mobility
5.
3-2-1 rule
• thyromentaldistance (distance of lower mandible in midline from the
mentum to the thyroid notch); <3 finger breadths (<6 cm) is associated
with difficult intubation
• mouth opening (<2 fingers is associated with difficult intubation)
• anterior jaw subluxation (<1 finger is associated with diffcult
intubation)
• A combination of the Mallampati score and thyromental distace is
the most accurate at predicting difficult intubation Anestnh
2005;103:429-437
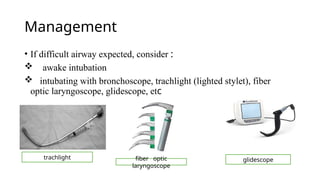
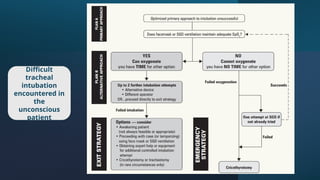
• If intubationunsuccessful after induction :
1. CALL FOR HELP
2. ventilate with 100% O2 via bag and mask
3. consider returning to spontaneous ventilation and/or waking patient
• If bag and mask ventilation inadequate:
1. CALL FOR HELP
2. attempt ventilation with oral airway
3. consider/attempt LMA
4. emergency invasive airway access (e.g. rigid bronchoscope,
cricothyrotomy, or tracheostomy
Clinical Significance
• Adifficult airway can become a life-threatening condition
very quickly if care is not taken to identify and prepare for this
eventuality properly.
• All practitioners responsible for intubating patients should be familiar
with the techniques.
• The abilities to ventilate, oxygenate, and maintain a patent airway are
crucial in patient survical.










































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


