
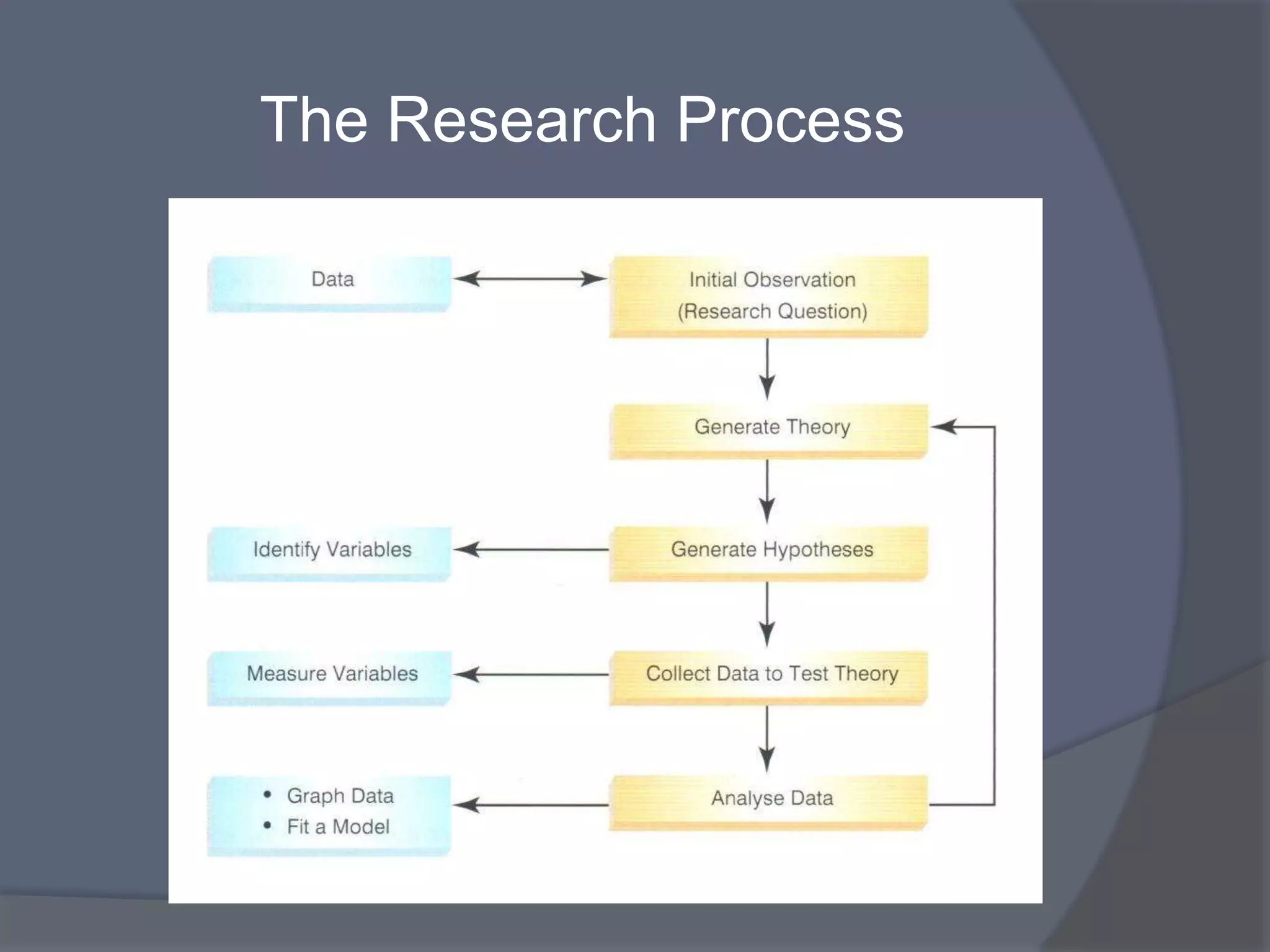

The document discusses research planning and methods. It describes identifying a knowledge gap and formulating a research question. Key aspects of a good research question are that it is important, innovative, answerable, and worth answering. The document contrasts background and foreground clinical questions. It emphasizes formulating questions focused on a specific problem, intervention, comparator, and outcome. Different study types - observational (descriptive, analytical) and interventional - are outlined, including their advantages and disadvantages. Cross-sectional, cohort, and case-control observational study designs are described in detail.








































































