Downloaded 35 times
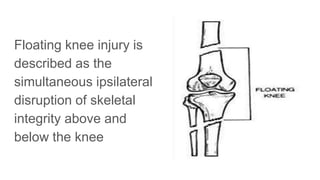









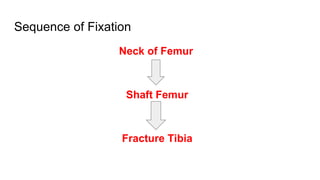
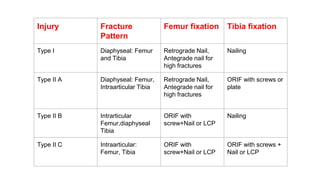







Floating knee injury refers to simultaneous fractures above and below the knee, usually from high-energy trauma like car accidents. These injuries have high rates of open fractures and associated injuries to other parts of the body. Treatment requires stabilization of both fractures while prioritizing any non-orthopedic injuries. Surgical fixation usually involves retrograde nailing of the femur followed by nailing or plating of the tibia. Ligament injuries are also common and may require MRI evaluation and treatment. Proper stabilization, treatment of associated injuries, and rehabilitation can lead to the best outcomes for these severe injuries.



































































