Downloaded 968 times







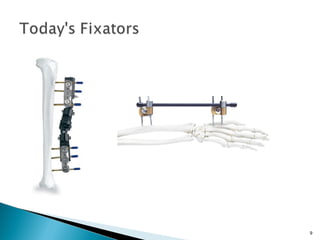











































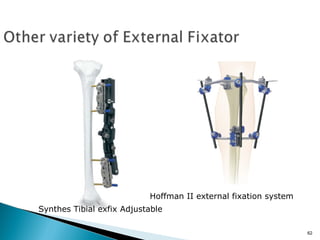



The document provides a history and overview of external fixators. Some key points: - External fixators were first developed in the 1840s and have since been improved, including the addition of threaded pins, rods, and adjustable clamps. - They are used to stabilize and immobilize long bone fractures, especially open or complicated fractures. - Components include Schanz pins, tubes, and universal clamps. Proper placement of pins is important for stability. - External fixators can be used temporarily to stabilize injuries before definitive fixation, or as the final fixation in cases where soft tissue healing is problematic. They provide less invasive fracture stabilization than internal fixation.