Downloaded 306 times
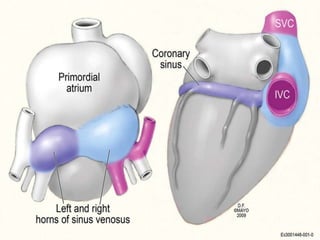
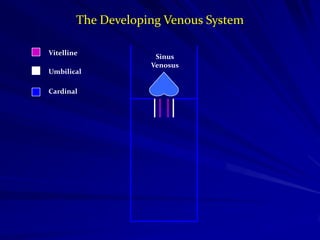
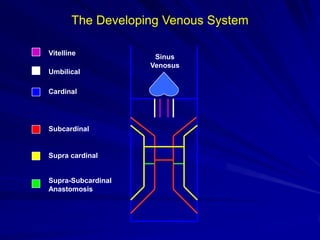
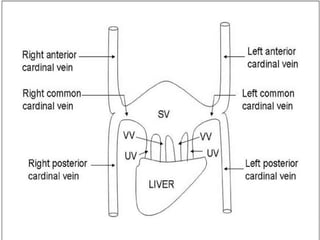
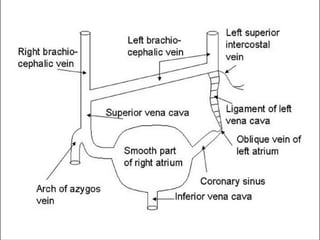
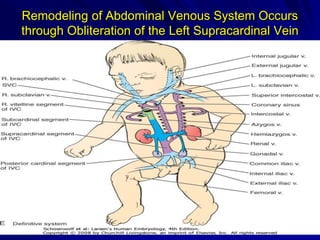
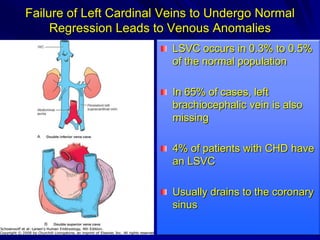
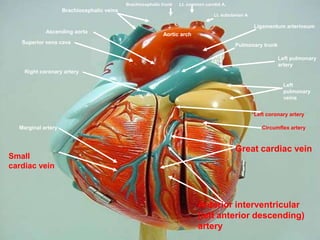

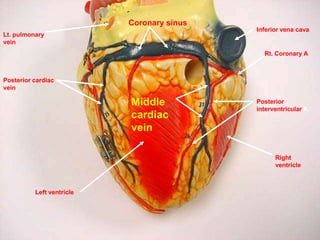
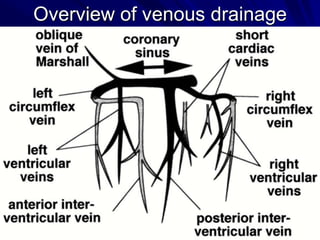




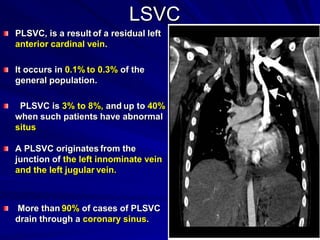
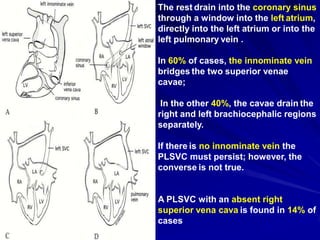
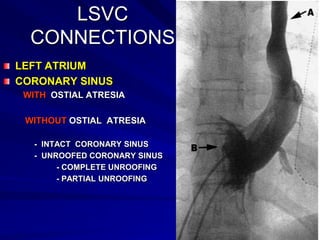
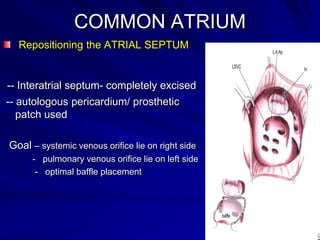

The document discusses the venous anatomy of the heart, including the coronary sinus and persistent left superior vena cava (LSVC). It begins with the embryological development of the venous system. It then describes the various tributaries that drain into the coronary sinus and provides an overview of the venous drainage patterns. It discusses surgical implications of anomalies such as LSVC connection variations, coronary sinus atresia, and partial unroofing of the coronary sinus.








































































































