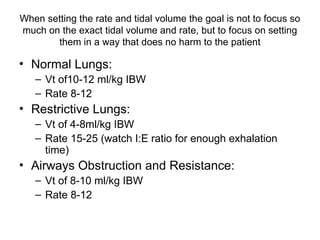
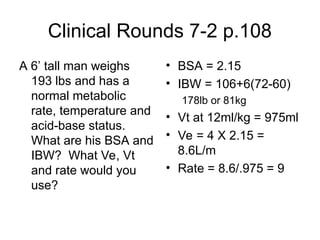
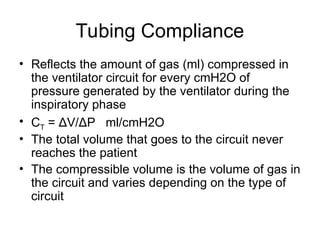
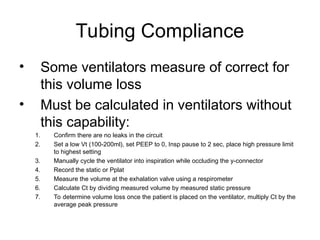
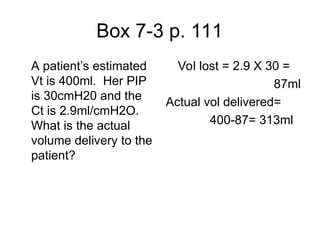
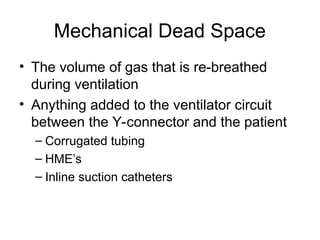
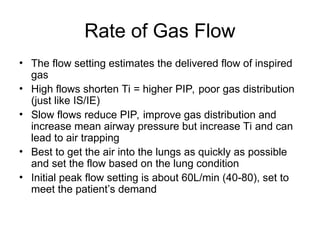
The document outlines initial ventilator settings for both volume and pressure ventilation, emphasizing tailored minute ventilation and tidal volume based on patient needs. It provides specific parameters for tidal volumes, rates, and the importance of adjusting settings based on lung mechanics, while also discussing tubing compliance and mechanical dead space. Additionally, the document covers techniques for monitoring and adjusting pressures in ventilation to ensure adequate gas exchange and minimize patient harm.