Downloaded 177 times
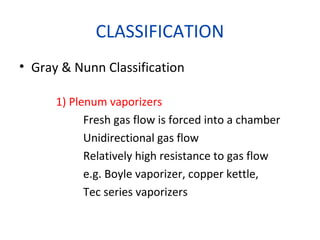



![EMO(ctd)
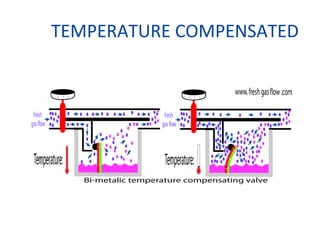
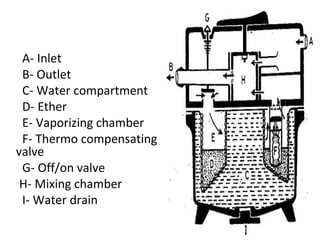
• Thermocompensation mechanism at outlet of
v.c.
– metal bellows with liquid Ether[ether capsule] &
connected to plunger
– temp. range; 15-29 degree Celsius
• Water jacket serves as heat reservoir
Checks
(1) check level indicator-> put “in transit”-> invert –
indicator should fall to full.
(2) close outlet- connect OIB to inlet-> put “in transit”->
press bellows-> open filler –no air should escape.
(3) release filler-set at 10% -rpt above
(4) attach bellows to outlet->block inlet –> set at 2 %
-suck air –> should hear a hissing if safety release
valve is working](https://image.slidesharecdn.com/vaporizers-150121125858-conversion-gate02/85/Vaporizers-2015-spmc-97-320.jpg)



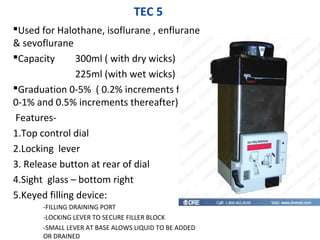
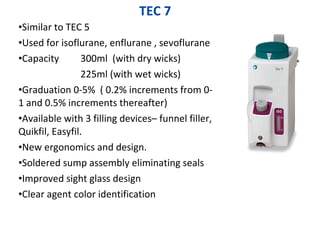












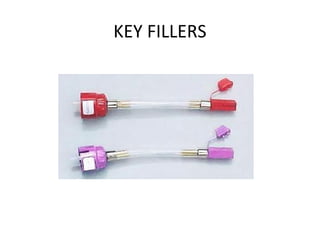



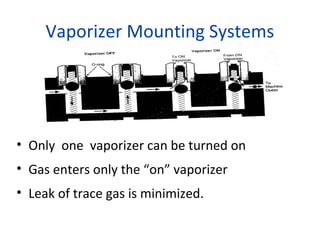



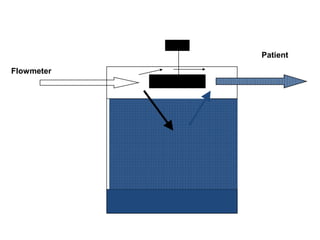
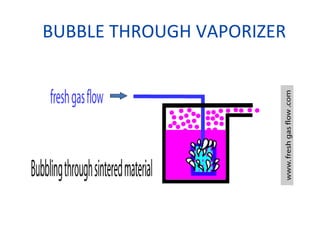
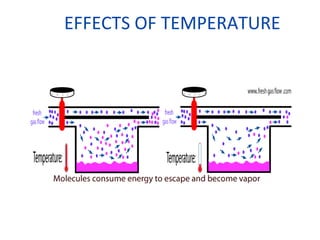
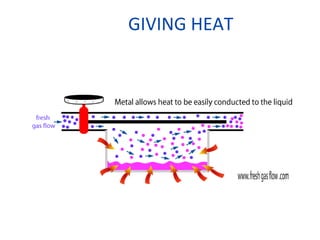
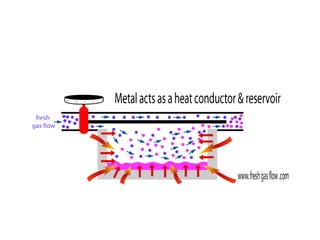
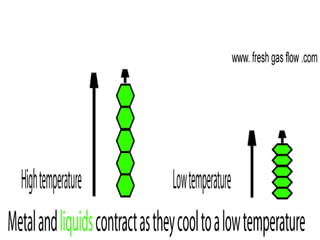
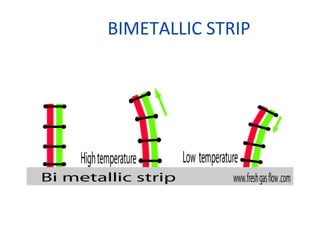
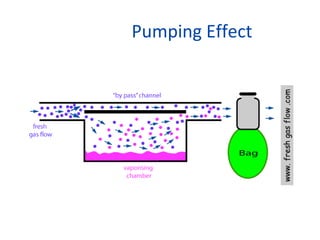
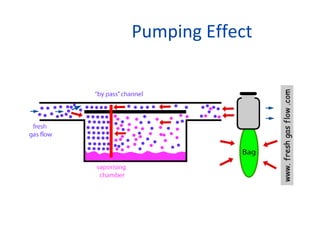
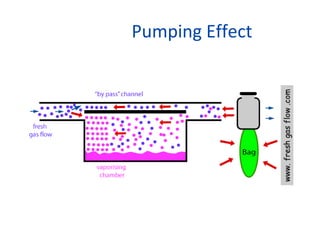
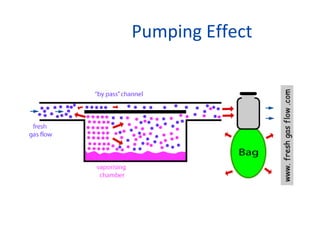
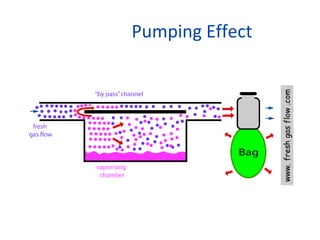
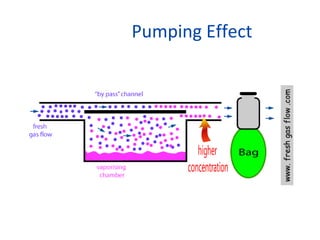
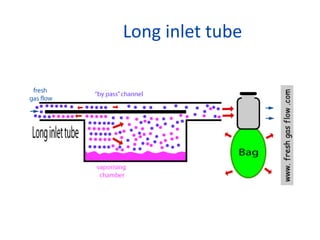
Vaporizers are instruments designed to facilitate the change of a liquid anesthetic agent into a vapor and add a controlled amount of this vapor to the fresh gas flow. They produce vaporization of volatile agents, mix the vapor with fresh gas, and control the mixture despite variables to safely and accurately deliver inhalational agents to patients. Vaporizer performance can be affected by factors like temperature, flow rate, barometric pressure, and intermittent back pressure, which vaporizer design and features aim to compensate for to maintain consistent agent delivery.





































![Vaporizer and Inhalational Anesthetics [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/vaporizerandinhalationalanestheticsautosaved-240829050532-cbdc4abd-thumbnail.jpg?width=640&height=640&fit=bounds)























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





