Thank you for the additional details on the Sarnat stages. This information helps provide more context for assessing and managing hypoxic ischemic encephalopathy in newborns.
Learning Outcomes
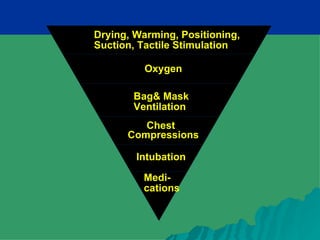
Initial Stabilisationand Resuscitation of the Newborn Infant
1. Prevention
1.1 Identify the factors that predispose to the development of
perinatal hypoxia.
1.2 Propose how perinatal hypoxia can be prevented.
2. Principles of Diagnosis
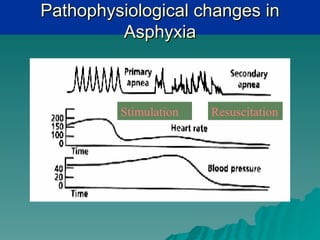
2.1 Describe the pathophysiological changes that occur in hypoxia.
2.2 Recognise an asphyxiated newborn
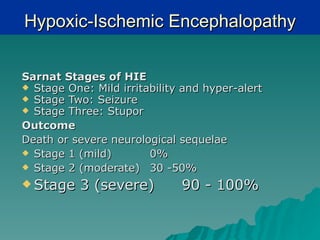
2.3 Classify an asphyxiated newborn based on the predicted
adverse outcomes (Sarnat staging)
3. Principles of Management
3.1 Resuscitate a newborn who is not adapting to the extra-uterine
transition.
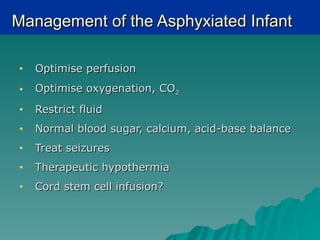
3.2 Describe the principles involved in the management of mild to
moderate asphyxiated newborn.
3.
Perinatal Hypoxia-Ischemia
Birth asphyxia - Failure to initiate
and sustain breathing at birth
Causes
5. Fetal and Antepartum (90%)
7. Birth process (10%)
4.
Fetal and AntepartumPathologies
1. Inadequate oxygenation of maternal blood
- anesthesia, cyanotic heart disease,
respiratory failure
3. Inadequate flow of maternal blood
(ischemia/hypotension) – spinal
anesthesia, compression of IVC or aorta
by uterus
5. Abruptio placentae
7. Uterine vasoconstriction (cocaine)
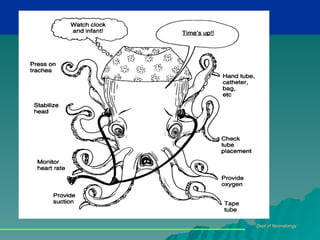
Recognition of anAsphyxiated Baby
Oxygen supply to the fetus is
reduced, resulting in
Apnea at birth
2. Low Apgar scores (severe if <5 at five
minutes)
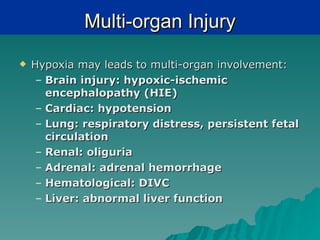
3. Neurologic sequelae (hypoxic-ischaemic
encephalopathy)
4. Metabolic acidosis
7.
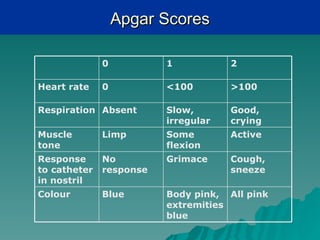
Apgar Scores
0 1 2
Heart rate 0 <100 >100
Respiration Absent Slow, Good,
irregular crying
Muscle Limp Some Active
tone flexion
Response No Grimace Cough,
to catheter response sneeze
in nostril
Colour Blue Body pink, All pink
extremities
blue
8.
Apnea
10 Apnea: When asphyxiated, the infant responds initially
with tachypnea. If insult continues, the infant becomes
apneic and bradycardic. The infant will respond to
stimulation and 02 therapy with spontaneous respirations.
20 apnea: When insult continues after 10 apnea, the infant
responds with a period a gasping respirations, bradycardia,
and falling BP. The infant takes a last breath and then
enters the 20 apnea period. The infant will not respond to
stimulation and death will occur unless resuscitation begins
immediately.
It is impossible to differentiate between 10 apnea and 20
apnea at delivery, assume the infant is in 20 apnea and
begin resuscitation immediately.
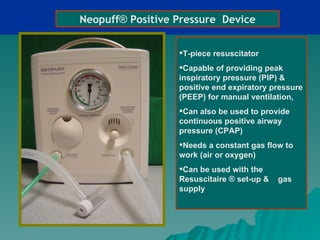
Neopuff® Positive PressureDevice
T-piece resuscitator
Capable of providing peak
inspiratory pressure (PIP) &
positive end expiratory pressure
(PEEP) for manual ventilation,
Can also be used to provide
continuous positive airway
pressure (CPAP)
Needs a constant gas flow to
work (air or oxygen)
Can be used with the
Resuscitaire ® set-up & gas
supply
24.
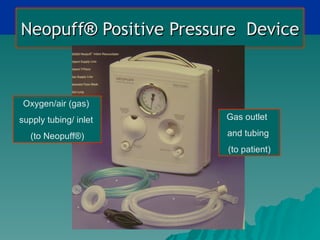
Neopuff® Positive PressureDevice
Oxygen/air (gas)
supply tubing/ inlet Gas outlet
(to Neopuff®) and tubing
(to patient)
25.
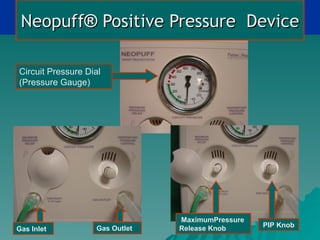
Neopuff® Positive PressureDevice
Circuit Pressure Dial
(Pressure Gauge)
MaximumPressure
Gas Outlet Release Knob PIP Knob
Gas Inlet
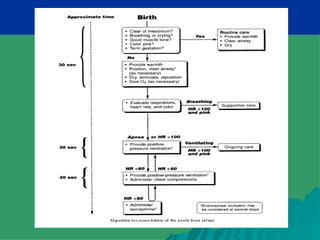
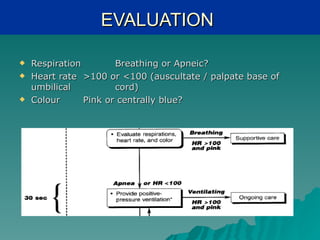
EVALUATION
Respiration Breathing or Apneic?
Heart rate >100 or <100 (auscultate / palpate base of
umbilical cord)
Colour Pink or centrally blue?
34.
POSITIVE PRESSURE VENTILATION
Indications: apnea / gasping, HR<100, persistent
cyanosis
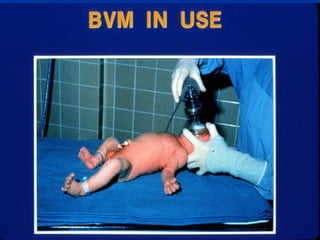
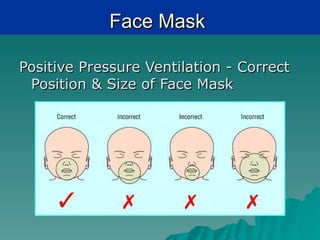
Bag and mask (self-inflating) with 100% O2
Adequate chest rise (rather than a particular
manometer reading)
Rate – 40 to 60 breaths per minute
Successful – improving HR and colour
The key to successful neonatal resuscitation is
establishment of adequate ventilation
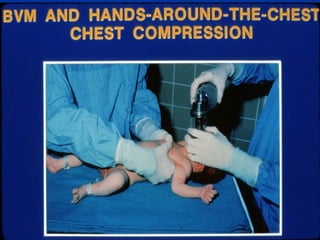
CHEST COMPRESSIONS
If after 30 seconds of adequate PPV with 100% O2 and
HR<60, start chest compressions
Ratio of 3 compressions : 1 breath, to give 90
compressions and 30 breaths per minute (120 events per
minute)
Depth of compression – 1/3 the depth of the chest
Preferred technique – Two thumb-encircling hands
Compressions delivered on the lower third of the sternum
39.
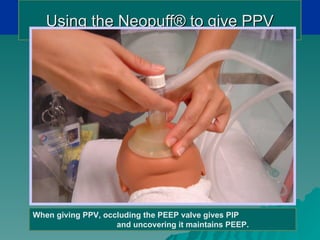
Using the Neopuff®to give PPV
When giving PPV, occluding the PEEP valve gives PIP
and uncovering it maintains PEEP.
40.
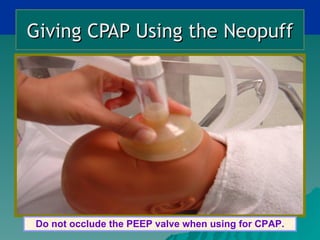
Giving CPAP Usingthe Neopuff
Do not occlude the PEEP valve when using for CPAP.
41.
Medications
1. Adrenaline
– Concentration 1 : 10 000 solution
– Dose 0.1 – 0.3 ml/kg
– Route ETT or intravenous
– Indication if HR < 60 bpm after 30 sec of effective PPV
and chest compressions
• Naloxone
– Dose 0.1 mg/kg, repeat dose if necessary
– Route intramuscular, intravenous, ETT
– For respiratory depression with maternal pethidine in
last 4 hours
3. Volume expanders (normal saline) 10 ml/kg over 10
minutes
5. Sodium bicarbonate
Case 1
You are asked to attend an emergency LSCS
delivery of a 41-weeks gestation infant with non-
reassuring fetal cardio-tocogram (CTG). Mother
is a 33 year old gravida one Chinese lady. She
was admitted to hospital two days ago. Her labor
was induced. She had good prenatal care and her
pregnancy has been uncomplicated. She suddenly
felt sharp pain in lower abdomen. CTG, which was
normal before that showed bradycardia.
47.
Case 1
Whatare the possible conditions that
you can think of in the mother
causing the problem?
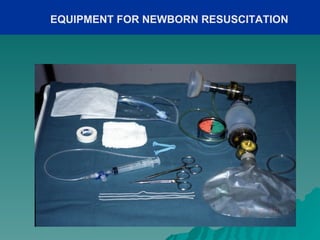
Whatresuscitation equipments would
you prepare for delivery?
Wouldyou involve any other medical
personnel?
48.
Case 1
Atdelivery,you receive a floppy and
blue male infant. His heart rate was
40/minutes and there is no
spontaneous respiration. Baby does
not respond to stimulation.
Whatis the initial Apgar score in this
baby?
What are the initial steps you would
49.
Case 1
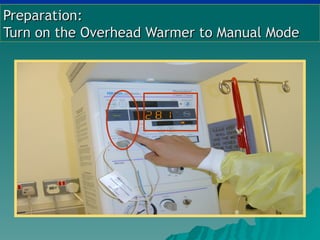
You bring him to the radiant warmer,
quickly positioned, dried, stimulated
the baby and give free-flow oxygen.
At 30 seconds of life, he remains
apneic and cyanotic. His heart rate is
still 40 per minute.
What would be the next step in
resuscitation?
50.
Case 1
Youadminister bag and mask
ventilation with 100% FiO2. There is
good chest expansion. After one
minute of bag and mask ventilation
baby remained apneic. His heart rate
is 60 per minute.
What would be your next step?
What are the other possible
51.
Case 1
Youstartchest compressions and
decide to intubate the baby.
How would you ensure proper
positioning of ETT?
How would monitor your
resuscitation?
52.
Case 1
You check for equal air entry and expansion of
lung field. Baby’s heart rate after two minutes of
ventilation is 100/minutes. The color is still pale
and pulse volume is low.
What could the possible reason for low volume
pulse?
What intervention would you like to consider at
this point?
53.
Case 1
You decide to give normal saline bolus 10-15
ml/kg.
How can you secure an intravenous access
quickly?
How fast do you want to administer the normal
saline bolus?
What are other types of fluid you can use?
54.
Case 1
Youcannulate the umbilical vein and
administer the normal saline over
five minutes. Baby’s heart rate
improve to 150/minute and color and
perfusion are better now. You have
decided to transfer the baby to
intensive care nursery.
Whatare the laboratory test you
want to order?
55.
Case 1
ABG shows following parameter
– pH 7.03
– PCO2 52 mm of Hg
– PO2 85 mm of Hg
– Base excess –15
– HCO3 12
– How would you interpret the ABG?
56.
Case 1
What are possible consequences in this baby?
– Clue: Organ systems
– Clue: Short term and long term
How would you monitor the baby?
– Symptoms
– Laboratory test
How would you counsel the parents regarding prognosis of
the baby?
57.
Case 2
You are requested to ‘stand-by’ for delivery of a
term neonate. The mother is 32-year- old. This is
her first pregnancy. Her antenatal follow-up was
irregular. She was admitted to hospital with labor
6 hours ago. The CTG shows persistent heart rate
of 170/minutes. Amniotic membrane was
ruptured spontaneously and it is heavily stained
with meconium.
58.
Case 2
Name few conditions that may give
rise to the problem described.
Whatare the resuscitation
equipments you would need?
Ideally,
how many medical personnel
you would need during resuscitation?
59.
Case 2
Thebaby is delivered vaginally. The
baby was found to covered with thick
meconium. There is no spontaneous
cry. The heart rate is 120/minute and
the baby has some activity.
What would the role of obstetrician?
What would be your first step in
resuscitation?
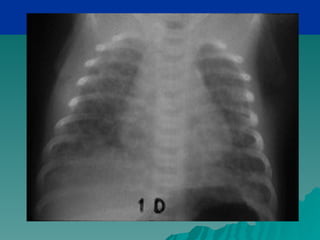
What are the consequences of
meconium aspiration?
61.
Conditions That RequiresDifferent
Resuscitation Approach
Thickmeconium stained liquor
Congenital diaphragmatic hernia
Feto-maternal or feto-placental
hemorrhage
62.
Reference and FurtherReadings
1. Neonatal resuscitation guidelines. Circulation
2005;112:118– 95.
• Volpe J. Neurology of the Newborn. 5 ed.
Philadelphia:W. B. Saunders Company; 2008
(Chapter on Neonatal Encephalopathy)
• Nelson Textbook of Pediatrics 18th ed. 2007
Chapter 99.5: Hypoxia-Ischemia















































![Neonatal resuscitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/neonatalresuscitationautosaved-210325082037-thumbnail.jpg?width=640&height=640&fit=bounds)


















![[Mary sheridan] from_birth_to_five_years_children(bookos.org)[1]](https://cdn.slidesharecdn.com/ss_thumbnails/marysheridanfrombirthtofiveyearschildrenbookos-200719030205-thumbnail.jpg?width=640&height=640&fit=bounds)



























