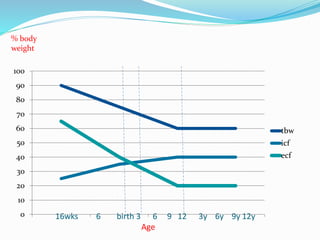
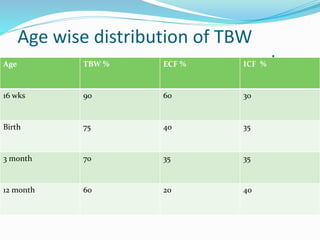
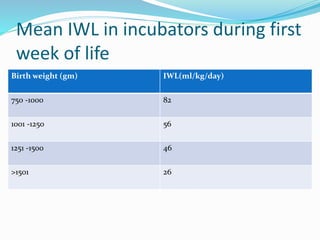
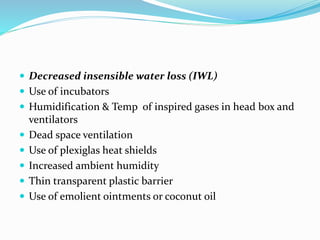
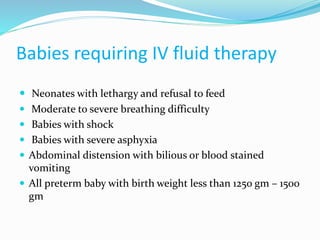
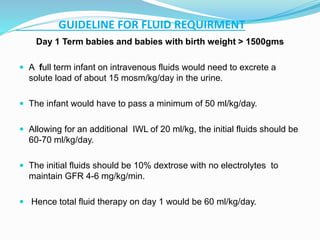
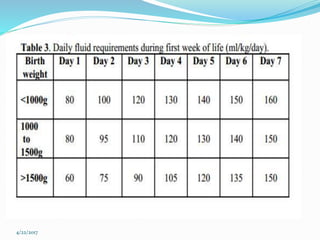
This document discusses fluid and electrolyte physiology in neonates. It covers developmental changes from intrauterine life through childhood and how this affects total body water, extracellular fluid, and intracellular fluid levels at different ages. It also discusses fluid shifts that occur during labor, delivery, and the postnatal period. Guidelines are provided for estimating insensible water loss and determining intravenous fluid and electrolyte requirements for term and preterm neonates of different gestational ages and weights.

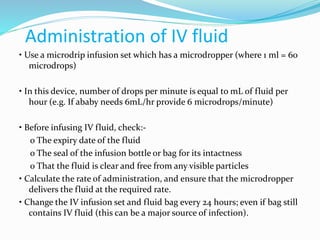
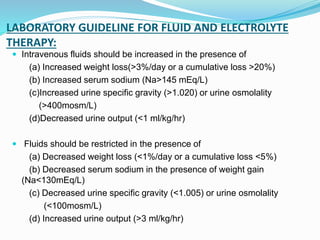
![Osmolality
Calculated osmolality
2 [Na+] + [Glucose] /18 + [BUN]/2.8
Effective osmolality /Tonicitiy
2[Na+] + [Glucose]/18
Calculated Osmolality –measured by degree of
freezing point depression](https://image.slidesharecdn.com/fluidelectrolytesmanagementinneonates-170422070717/85/Fluid-electrolytes-management-in-neonates-13-320.jpg)


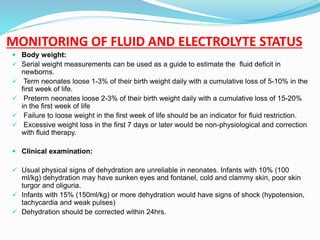
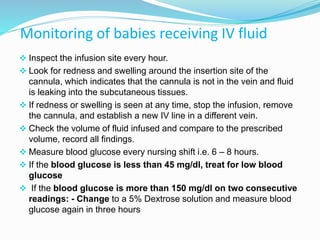
![ Blood gas:
Useful in the acid base management of patients with poor
tissue perfusion and shock.
Hypo-perfusion is associated with metabolic acidosis.
Fractional excretion of sodium (FENa):
Reflects the balance between GFR & tubular
reabsorption of Na but is of limited value in preterm
infants due to developmental tubular immaturity
FE Na+ =Urine [Na] x Serum Creatinine
Serum [Na+] x Urine Creatinine x100%](https://image.slidesharecdn.com/fluidelectrolytesmanagementinneonates-170422070717/85/Fluid-electrolytes-management-in-neonates-52-320.jpg)















































![fluid_and_electrolytes[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fluidandelectrolytes1read-only-250903084601-61978d1f-thumbnail.jpg?width=640&height=640&fit=bounds)


























