
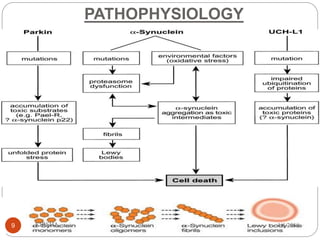
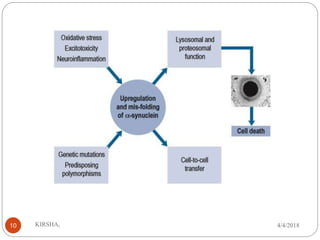
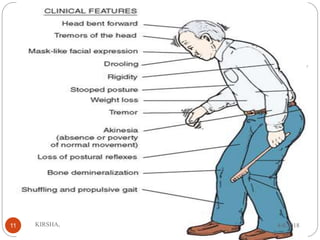
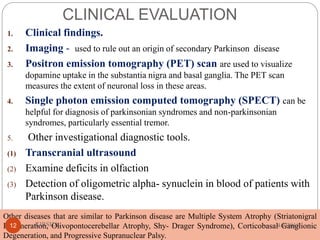


Parkinson's disease is a progressive neurological disorder that causes tremors, rigidity, and slowed movement. It results from the loss of dopamine-producing neurons in the substantia nigra. Primary Parkinson's has no known cause while secondary Parkinsonism can be caused by drugs, toxins, infections, or other neurological conditions. Symptoms are treated pharmacologically with levodopa and other dopamine agonists to replace lost dopamine, though no treatment can stop the progression of the disease. Advanced cases may be treated with surgery such as deep brain stimulation.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







