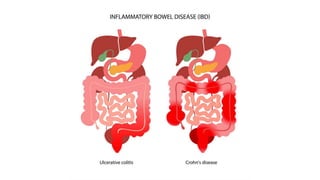
3. Classification of inflammatory bowel disease
• Inflammatoryboweldisease(IBD) isanumbrella termfor twochronic inflammatorydisorders
of thegastrointestinalsystem:
-Ulcerative colitis(UC)
-Crohn’sdisease(CD)
4. Clinical presentation of ulcerative colitis
Recurrent attacks of inflammation and ulcers in the colon and rectum
5. -Onset : isgradual andinsidious,maybeacute
-Peak age of onset :30to40 years
-Bloody diarrhea
-Frequent stools
-Mucous discharge
-Urgency to defecate
-Tenesmus
-Periods of remission and relapse
-Extracolonic manifestations include: musculoskeletal, cutaneous, ocular andhepatobiliaryconditions
Clinical presentation of ulcerative colitis
6. Clinical presentation may vary based on the type
-Rectal bleedingmaybetheonly
sign
-Maypredominantlyhaveurgency
andtenesmus
-Bloody diarrhea
-Abdominal cramps and pain
-Tenesmus
-Bloodydiarrhea
-Abdominal cramps andpain on theleft
side
-Urgency todefecate
-Bouts ofbloodydiarrhea
-Abdominal cramps and pain on theleft
side
-Fatigue
-Significant weight loss
8. -Mild cases: may be normal except mild tenderness in lower left abdominal quadrant
-Moderate to severe cases: abdominal tenderness and cramps
-Severe cases: fever- tachycardia- significant abdominal tenderness- weight loss
-Fulminant course: severe diarrhea and cramps- fever- leukocytosis- abdominal distention
9. The age of the patient: 28
Onset and course: episodesexperiencedoverthepast 6to8months with remission, recentexacerbation of2days
Symptoms: frequent stools (10 to 12 times) , blood and mucous, small volume, urgency to defecate
Abdominal painwith mildlydistended abdomen, diffusetendernessand hypoactivebowel sounds
Clinical presentation suggestive of ulcerative colitis in the case
Temperature: 38
Heart rate: 110
Leucocytosis: 15,800
Hemoglobin: 10.3
Platelet count: 754,00
10. Ulcerative colitis Crohn’s disease
Wall Mucosal , submucosa ulcers Transmural inflammation
knife like fissured
Site Large intestine , usually rectum usually ilium
Lesion Continuous mucosal Interrupted , skip lesions
C/P LLQ + bloody diarrhea RLQ + - bloody diarrhea
Mscope Crypt abscess
Neutrophils
Non caseating granuloma
Gross loss of haustration
pseudo polyps
Cobblestone mucosa *
creeping fat , stricture
Complications Toxic megacolon *
colon cancer
Malabsorption ( b12 )
Ca stones* , Fistula , stricture
Imaging Lead pipe String sign
14. site Extraintestinal manifestations
Hepatopancreatobiliary system •Primary sclerosing cholangitis, bile-duct carcinoma
•Associated inflammation: autoimmune chronic active hepatitis,
pericholangitis, portal fibrosis, cirrhosis, granulomatous disease
•Metabolic manifestations: fatty liver, gallstones associated with ileal Crohn's
disease
Ocular system •Uveitis/iritis, episcleritis, scleromalacia, corneal ulcers, retinal vascular
disease
Metabolic system •Growth retardation in children and adolescents, delayed sexual maturation
Renal system •Calcium oxalate stones
15. Diagnostic tools for IBD
• 1-Approach :
• Evaluate patients with hematochezia and fecal urgency for
ulcerative colitis.
• Rule out infectious gastroenteritis.
• Consult gastroenterology for ileocolonoscopy with histological
examination
• Consider CT or MRI abdomen if direct endoscopy is contraindicated.
16. 2-Lab studies
• Stool testing for causes of gastroenteritis is indicated in all patients. Blood
tests are not routinely required for diagnosis but help assess disease
activity and severity.
• Blood tests
• CBC: anemia, leukocytosis, thrombocytosis [4]
• ESR, CRP: Elevated levels may indicate active ulcerative colitis and
often correlates with disease severity.
• Hypoalbuminemia
• ALP, GGT: elevated in patients with concurrent PSC
• Perinuclear ANCA (pANCA) [2]
• Not routinely recommended
• Elevated in up to 70% of patients with ulcerative colitis
• Stool diagnostic studies
• Stool test for Clostridioides difficile infection
• PCR panel for other enteric infections: depending on the patient's
symptoms and risk factors for diarrhea
• Stool culture and microscopy: to assess for bacteria
and ova and parasites if a stool PCR panel is not available
• Fecal calprotectin: can help assess for mucosal inflammation
18. Acute ulcerative colitis
Colonoscopy photo of sigmoid colon
The mucosa is erythematous and edematous
indicating active inflammation . There is loss
of superficial vascular markings and linear
semi-confluent ulcerations.
20. Ulcerative colitis in
remission
Colonoscopy photograph .
No signs of acute inflammation are visible.
Some loss of haustra and vascular markings
as a result of previous exacerbations can be
seen.
21. 4-Imaging
• Imaging studies are not routinely recommended for diagnosing ulcerative colitis but may be used as an adjunct to
endoscopy, particularly for the detection of complications, or if endoscopy is not possible. [4]
• 1-Abdominal x-rays [2][4][17]
• Indication: initial and serial evaluation of suspected ASUC
• Findings
• Typically normal in mild-to-moderate disease
• Loss of colonic haustra (lead pipe appearance) may be seen in severe cases
• May show signs of complications, e.g.:
• Toxic megacolon: massive distention
• Ulceration: segmental dilation with irregular edges outlined by gas [17]
• Perforation: pneumoperitoneum [18]
24. Complications
Possible complications of ulcerative colitis include:
• Severe bleeding
• Severe dehydration
• A rapidly swelling colon, also called a toxic megacolon
• A hole in the colon, also called a perforated colon
• Increased risk of blood clots in veins and arteries
• Inflammation of the skin, joints and eyes
• An increased risk of colon cancer
• Bone loss, also called osteoporosis