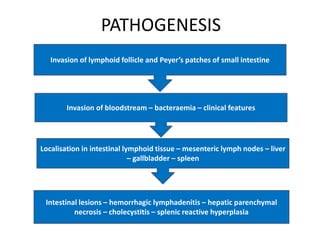
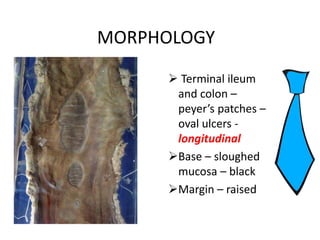
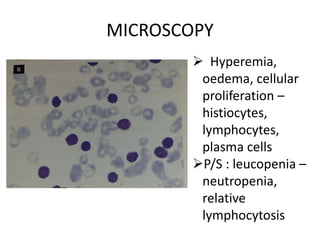
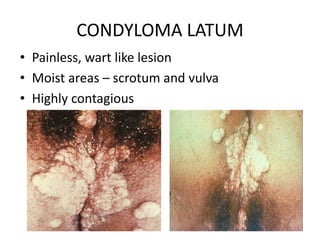
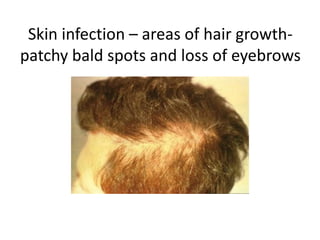
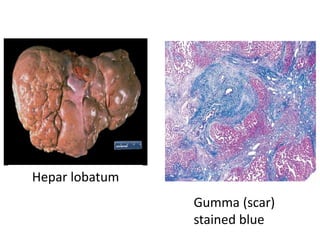
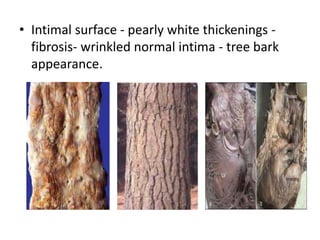
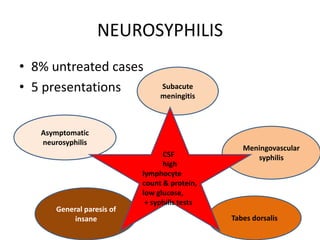
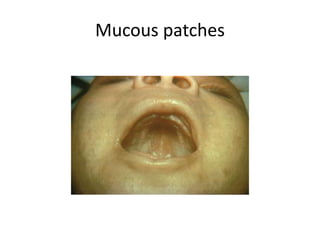
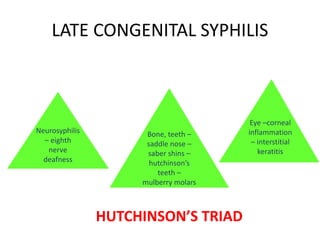
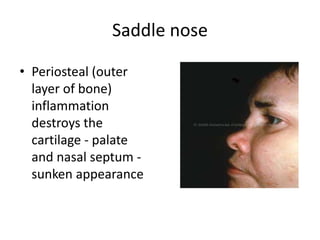
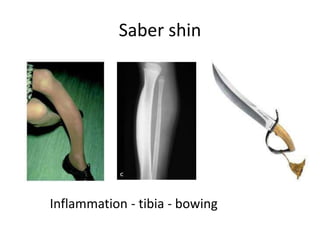
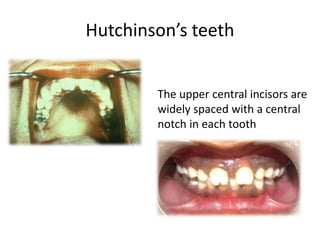
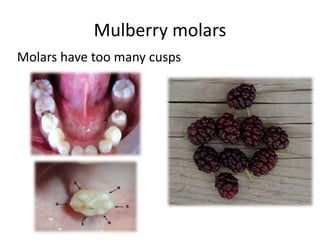
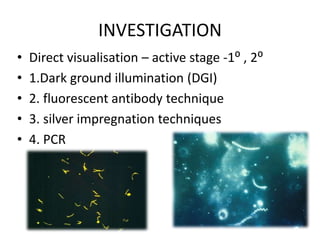
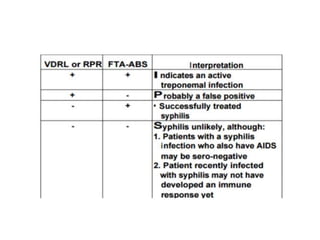
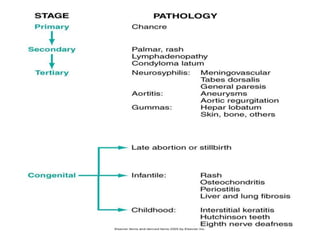
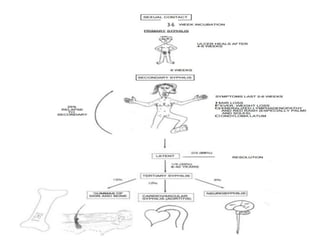
This document discusses typhoid and syphilis. It begins by presenting a case scenario of a man experiencing abdominal pain, nausea, vomiting and fever who may have typhoid fever based on his recent consumption of undercooked eggs. It then provides details on the pathogenesis, clinical features, investigations and treatment of typhoid fever. The document also presents a case of a man with a penile sore and lymphadenopathy who is diagnosed with primary syphilis. It outlines the stages, signs and symptoms, histology, and management of syphilis.