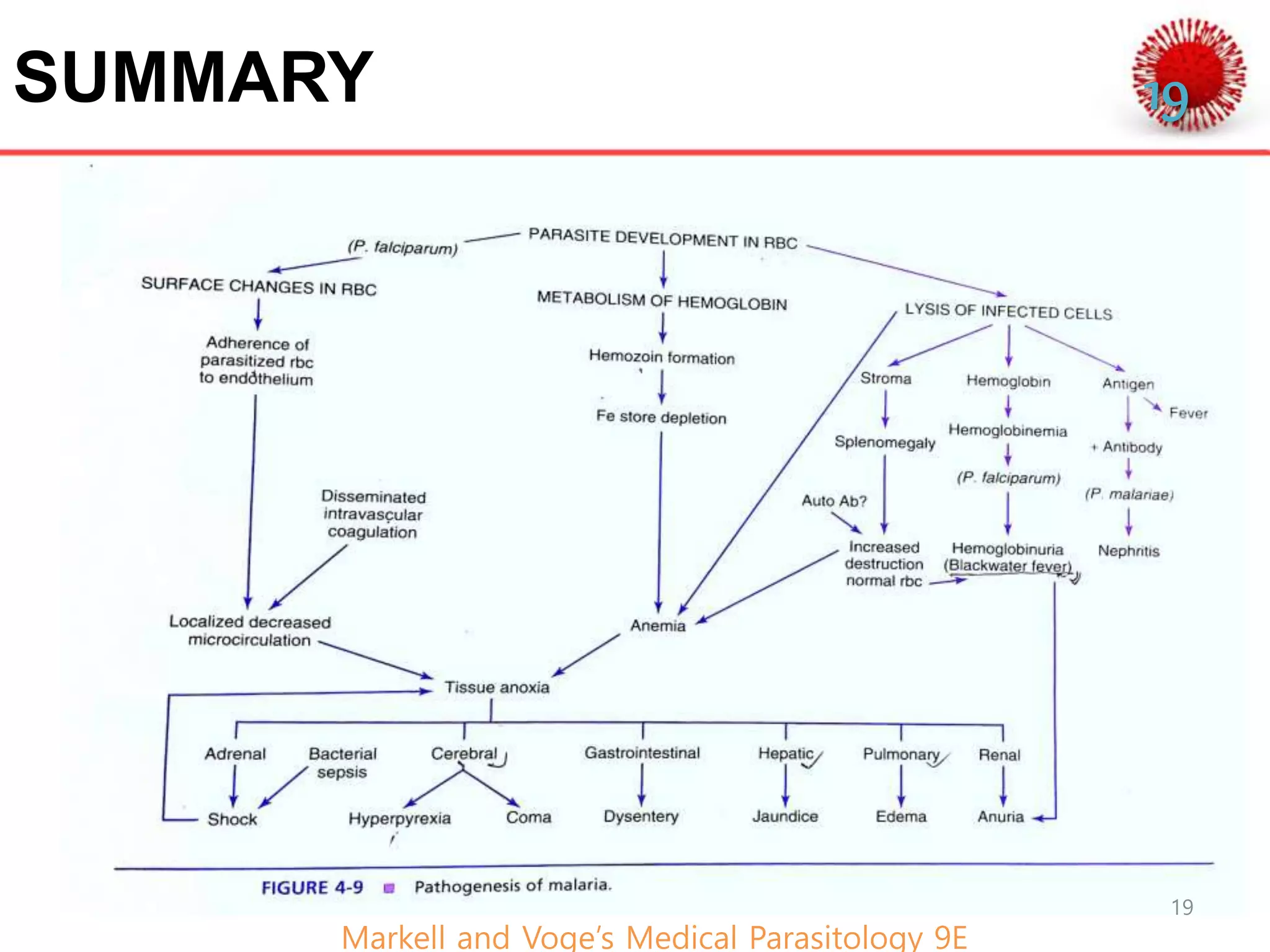
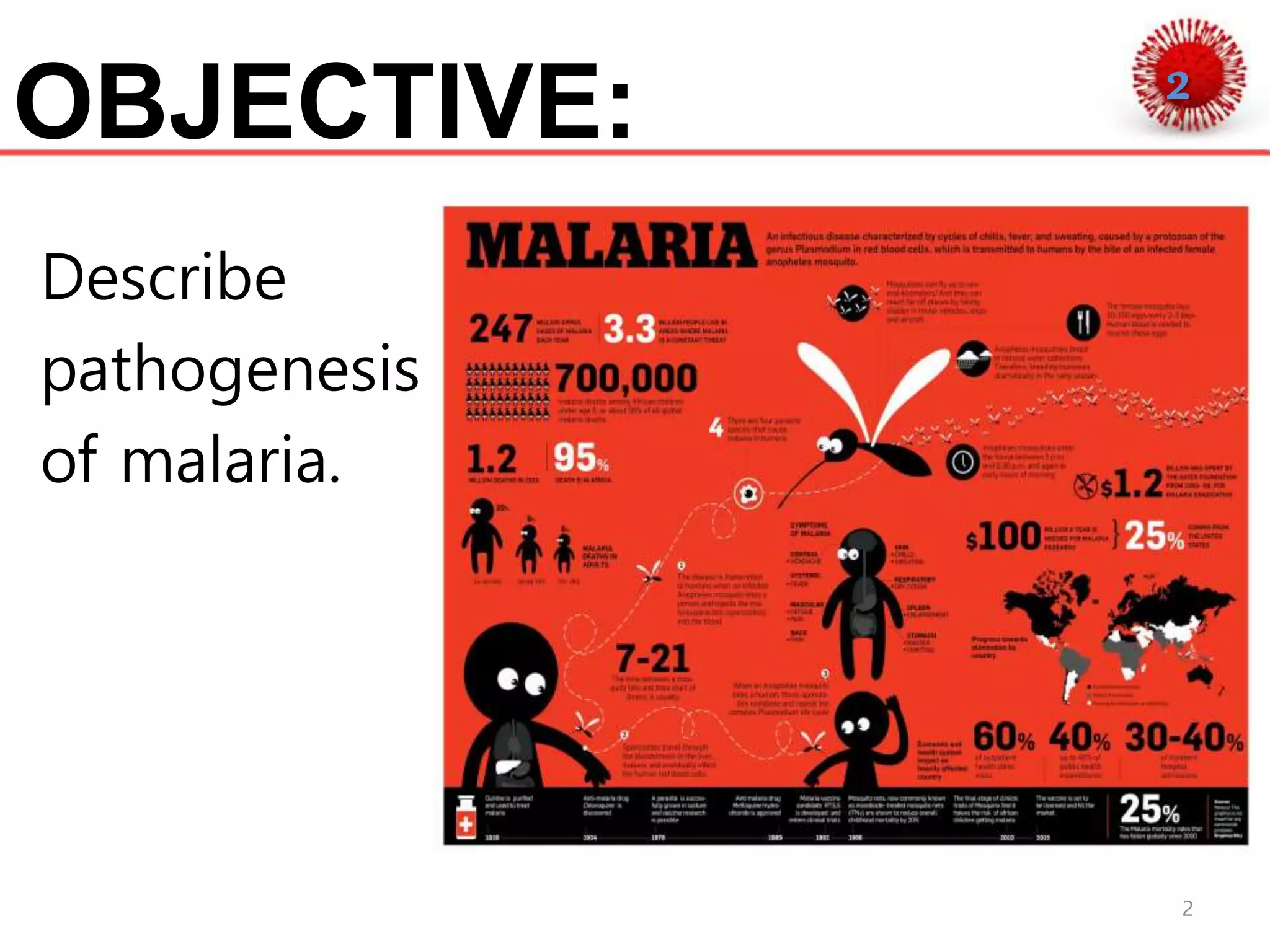
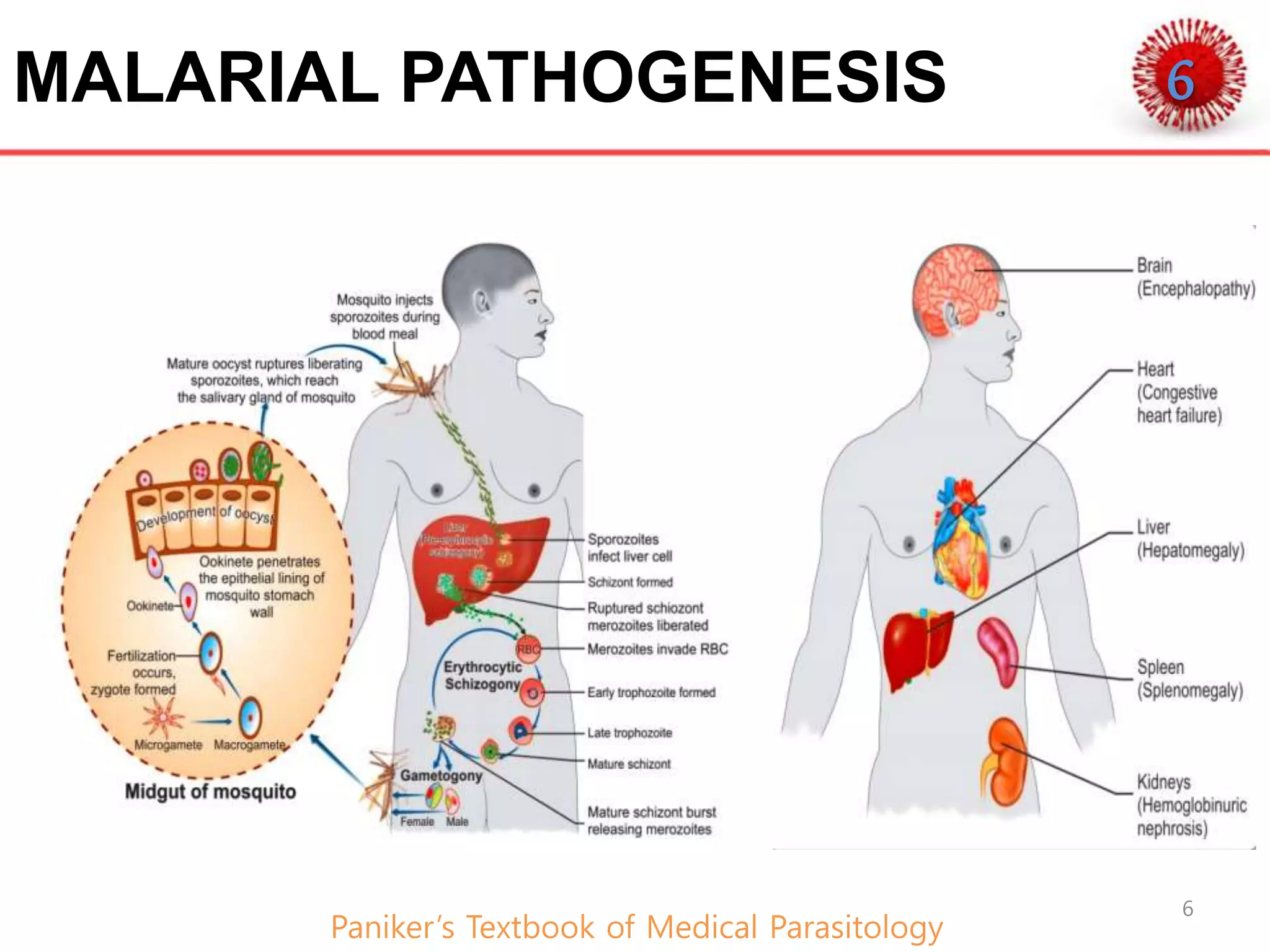
Malaria is a vector-borne infectious disease caused by protozoan parasites of the genus Plasmodium. It is transmitted via the bites of infected female Anopheles mosquitoes and causes approximately 219 million cases and 435,000 deaths worldwide annually. Younger children, pregnant women, and immunocompromised individuals are most at risk. The pathogenesis involves hepatic and erythrocytic phases where the parasites multiply and rupture red blood cells, releasing toxins and cytokines that cause fever, chills, and other symptoms. In severe malaria caused by P. falciparum, infected red blood cells bind to endothelial cells of small blood vessels, blocking blood flow and damaging organs.




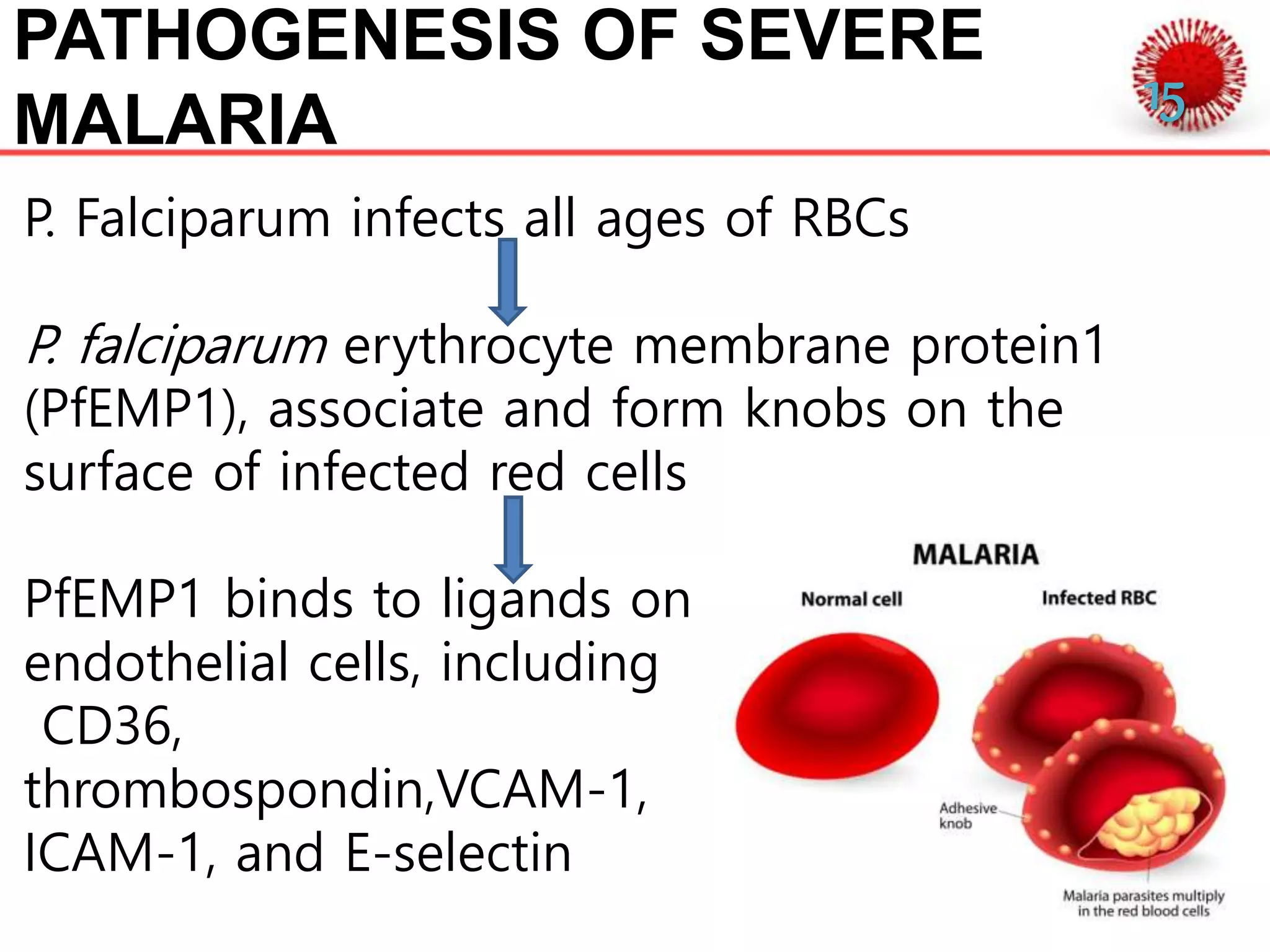
![PATHOGENESIS OF SEVERE
MALARIA
Infected RBCs to clump
together(ROSETTE)
Stick to endothelial cell lining
of small blood vessels
(SEQUESTRATION)
Blood flow blocks which
decreases tissue perfusion
and leads to Ischemia
[Manifestation of cerebral malaria] Robbins and Cotran
Pathologic Basis of diseases
SAE
16](https://image.slidesharecdn.com/pathogenesisofmalarial-190702213458/75/Pathogenesis-of-malaria-16-2048.jpg)