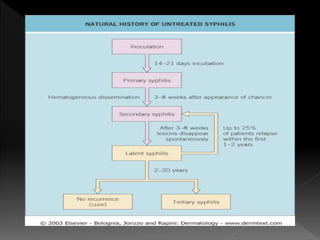
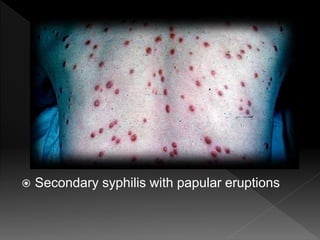
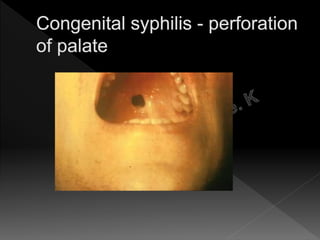
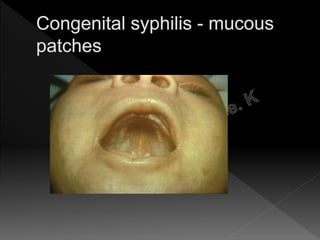
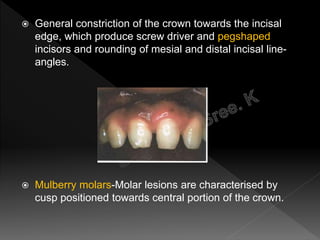
Syphilis is a chronic infectious disease caused by the bacterium Treponema pallidum. It has various stages including primary, secondary, and tertiary syphilis. Primary syphilis involves a chancre sore, secondary syphilis a rash and mucous patches, and tertiary syphilis can include gummas or neurosyphilis. Syphilis is diagnosed through tests like dark-field microscopy, VDRL, and FTA-ABS. Treatment is with antibiotics. Congenital syphilis occurs when a fetus is infected in utero, which can cause rhagades, osteitis, or 8th nerve deafness in the infant.