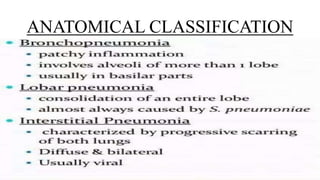
The document provides a comprehensive overview of pneumonia, including its definition, risk factors, types (community-acquired, hospital-acquired, and aspiration pneumonia), and the underlying pathophysiology. It outlines clinical manifestations, diagnostic methods, medical and nursing management, and preventive measures. Additionally, it discusses potential complications such as respiratory failure, empyema, sepsis, and acute respiratory distress syndrome (ARDS).