
















































































































This document provides an overview of the immune system, including its history, components, and functions. It discusses the types of immunity, including innate, humoral, and cell-mediated immunity. It describes the key players in the immune system like antigens, antibodies, and the complement system. It explains the mechanisms of the antigen-antibody reaction, including precipitation, agglutination, complement fixation, immunofluorescence, and radioimmunoassay. The immune system provides protection from infection through physical barriers, antimicrobial factors, inflammation, and adaptive immune responses mediated by antibodies and specialized immune cells.
Overview of immune system components and functions including antigen, antibody, immunity types, and diseases.
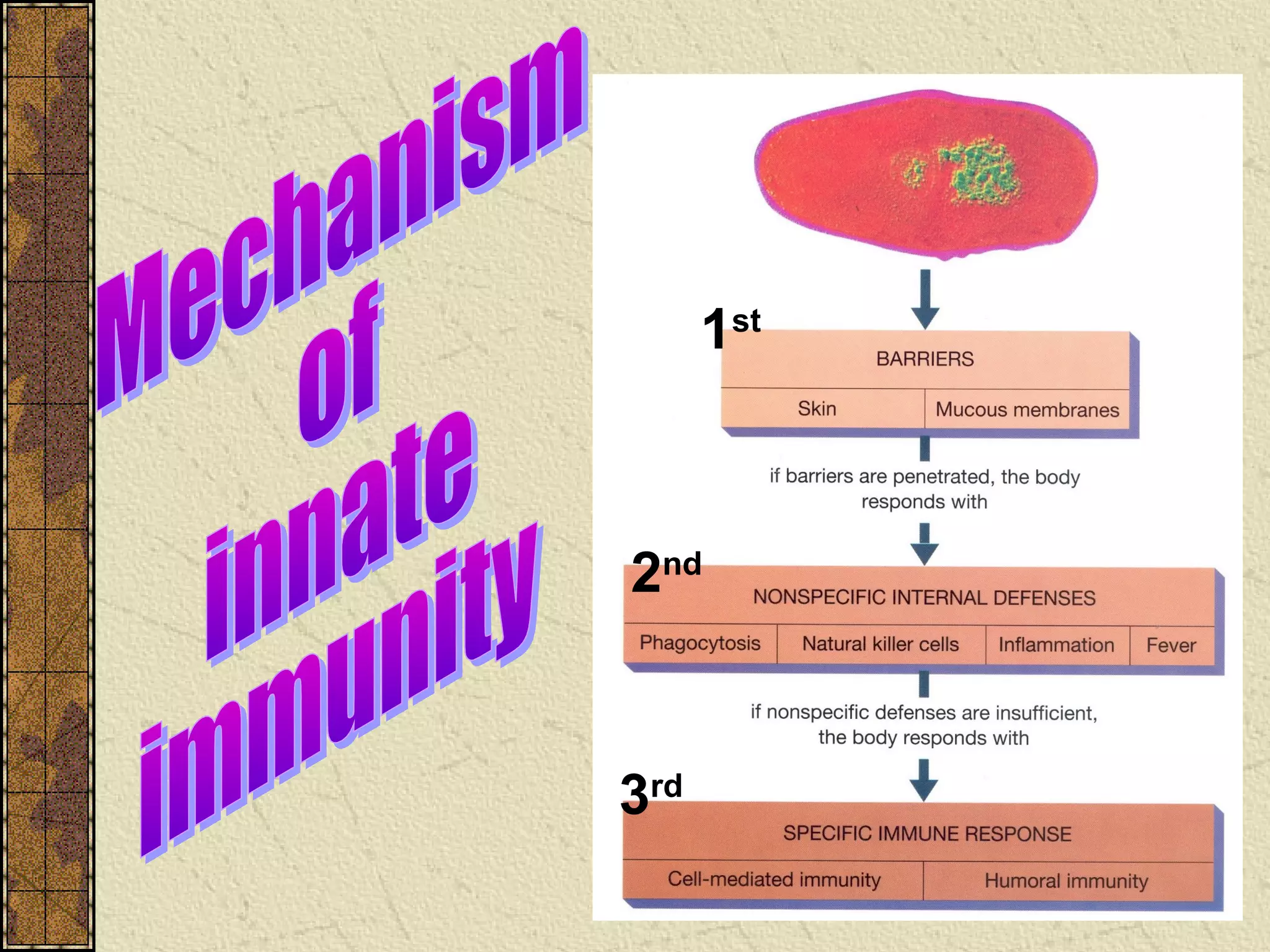
Impact of microbes on health and the immune system's role in combating infections, immunity definitions, and defense layers.
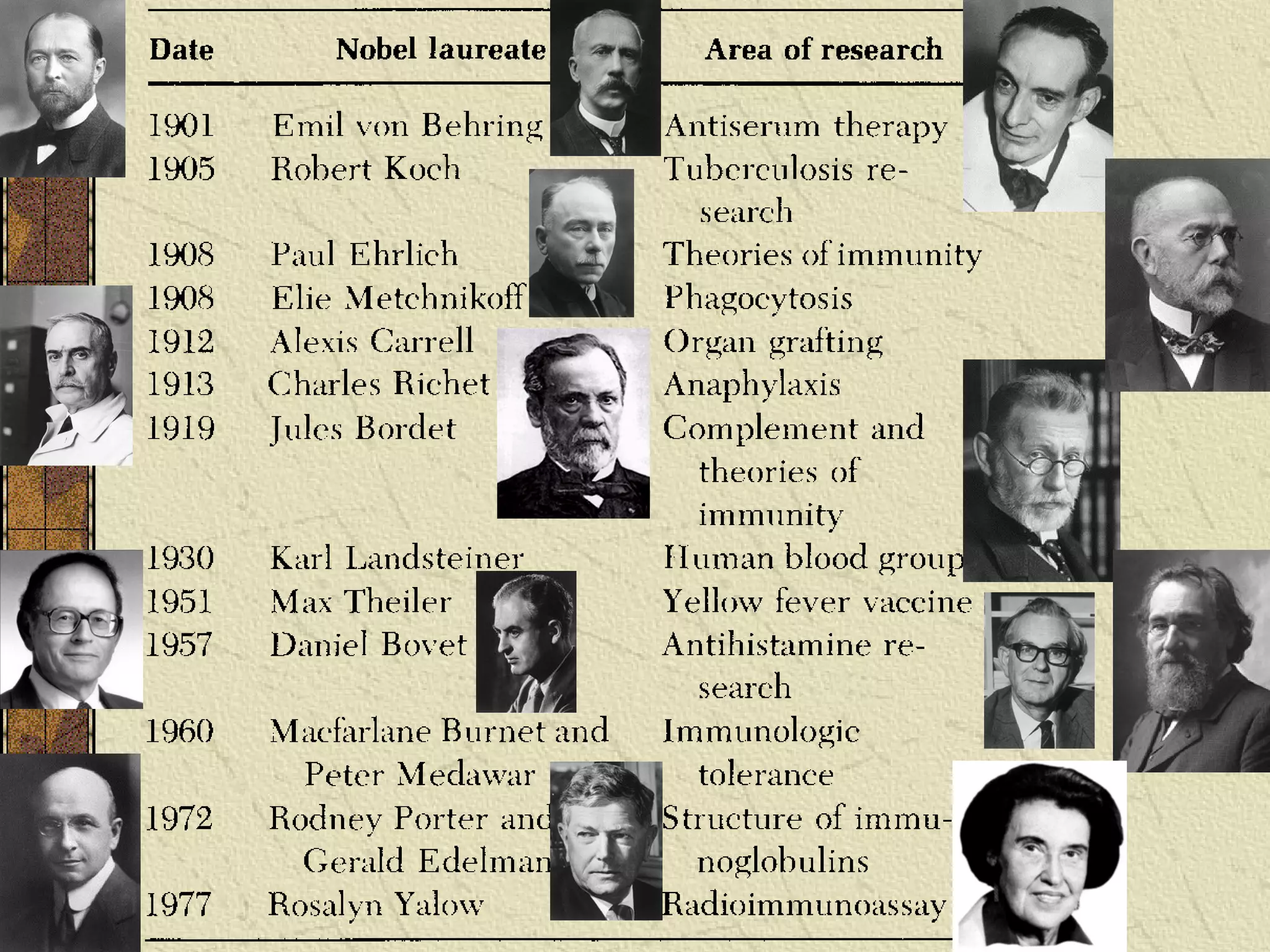
Influential scientists in immunology including Jenner, Pasteur, Koch, and their contributions to vaccine development.
Concept of immunity likened to an army's defense strategy, and detailing innate and various influencing factors.
First line defenses including epithelial surfaces, antimicrobial substances in blood, and cellular defenses in the immune system.
Description of inflammation as a defense mechanism and the role of fever in combating infections.
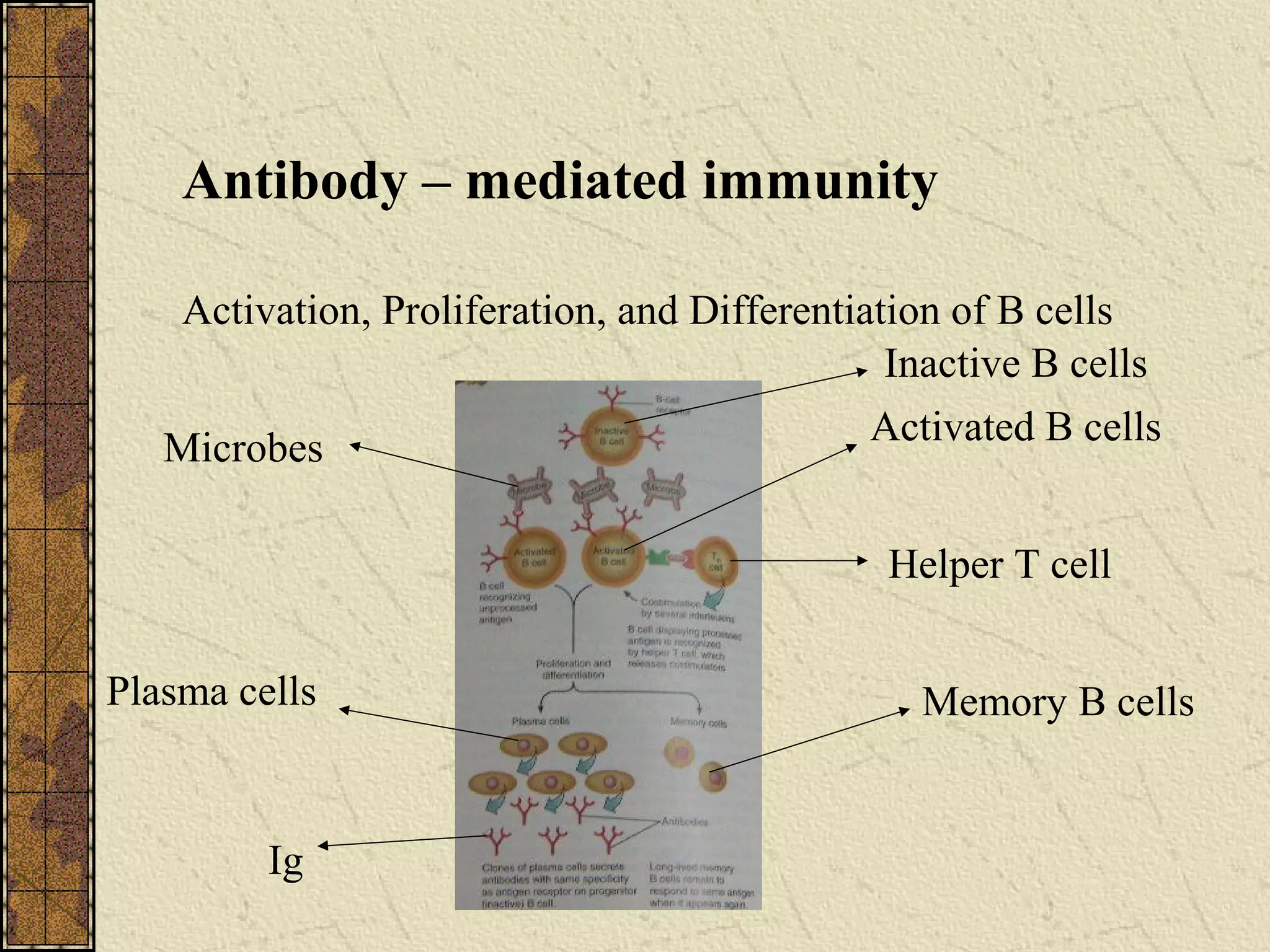
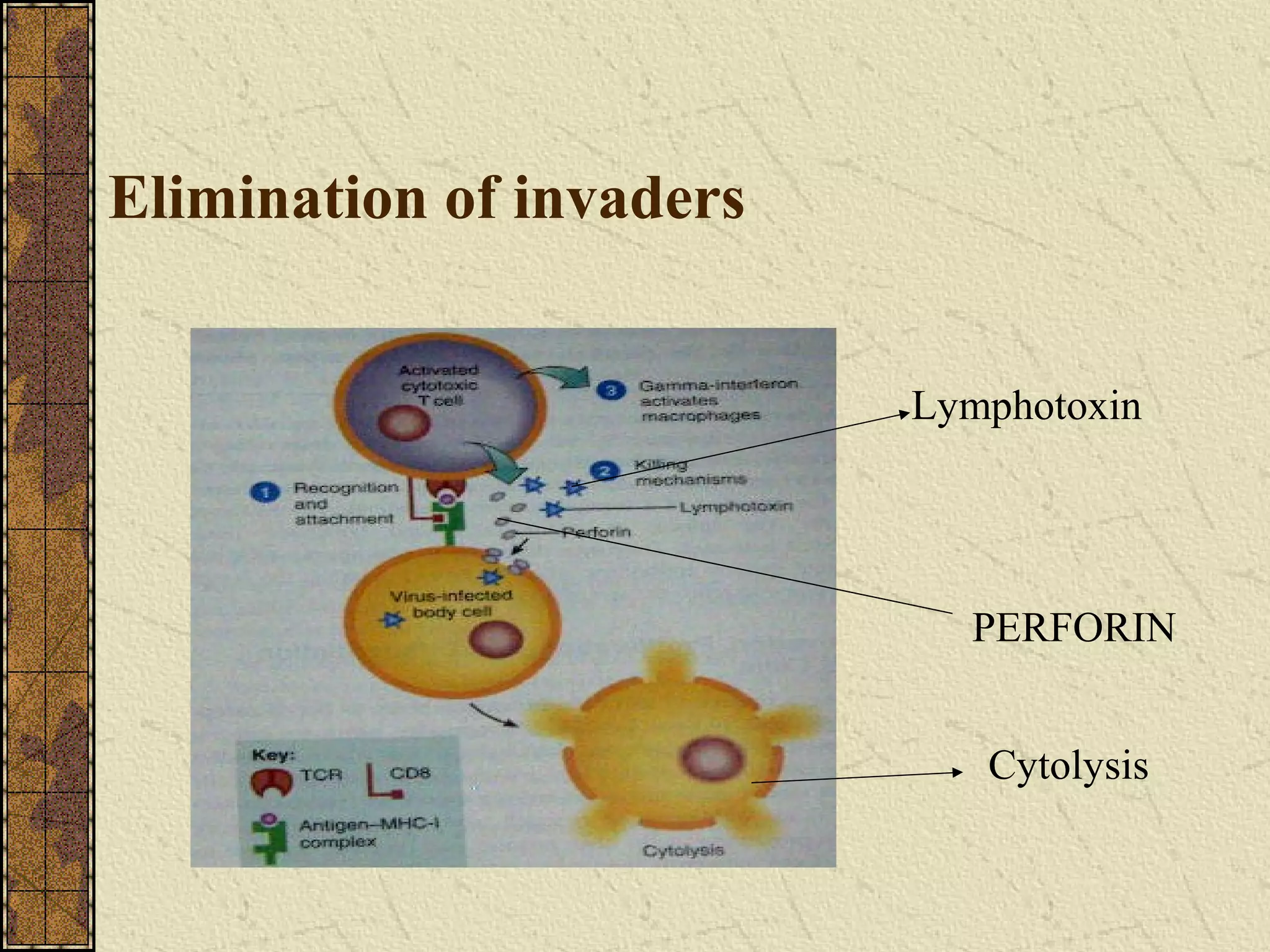
Details on humoral and cell-mediated immunity, including the differences between active and passive immunity.
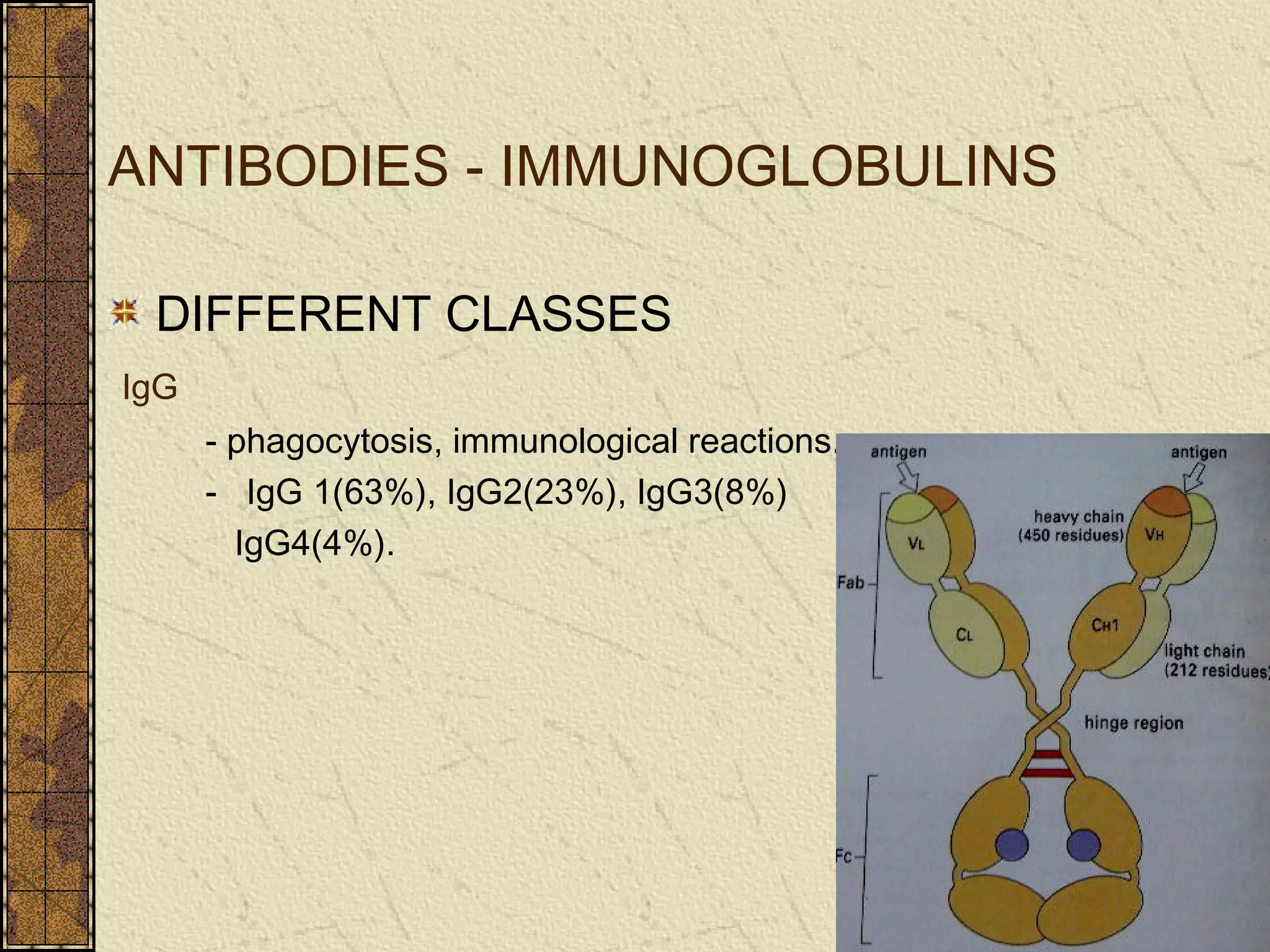
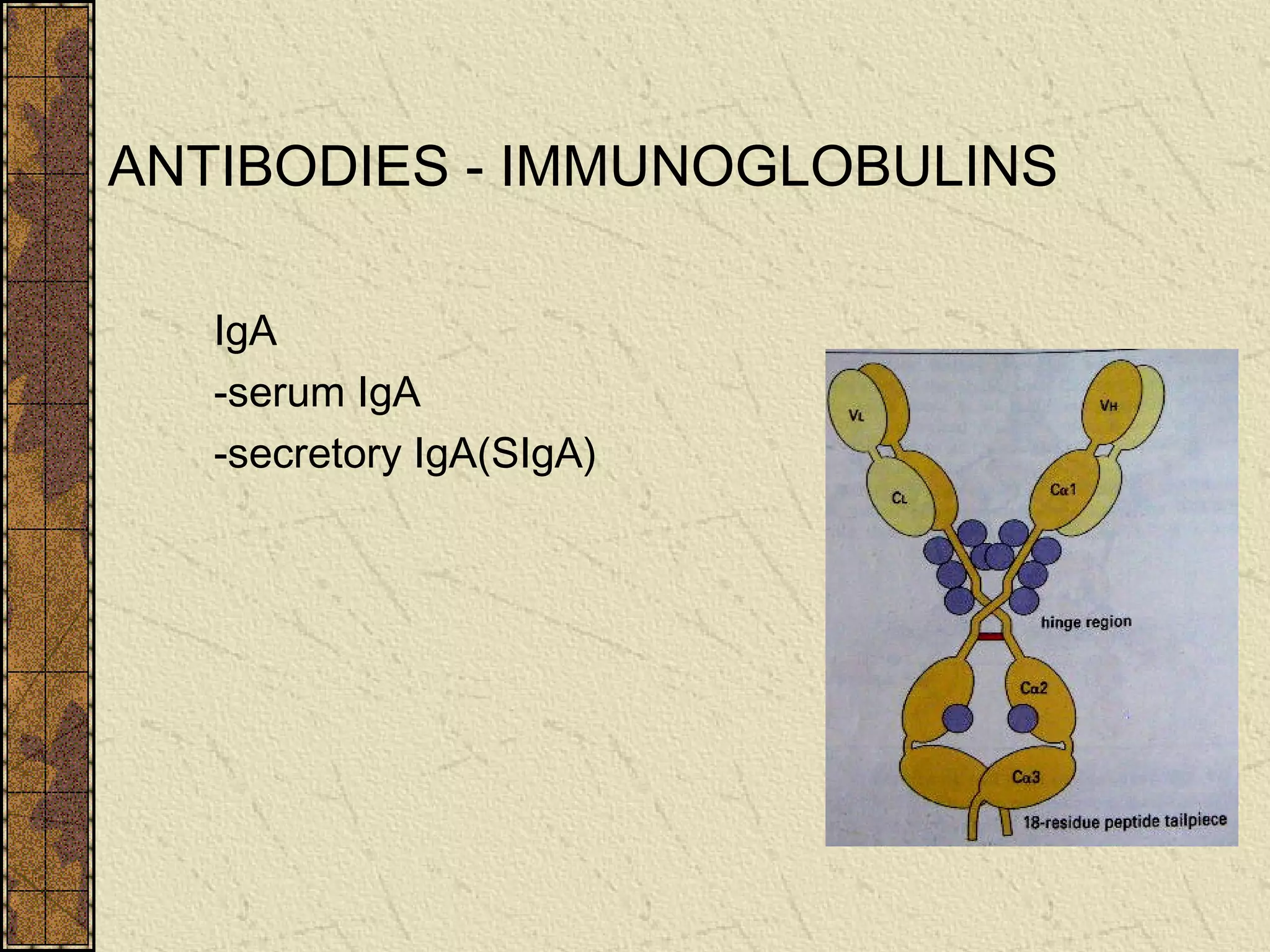
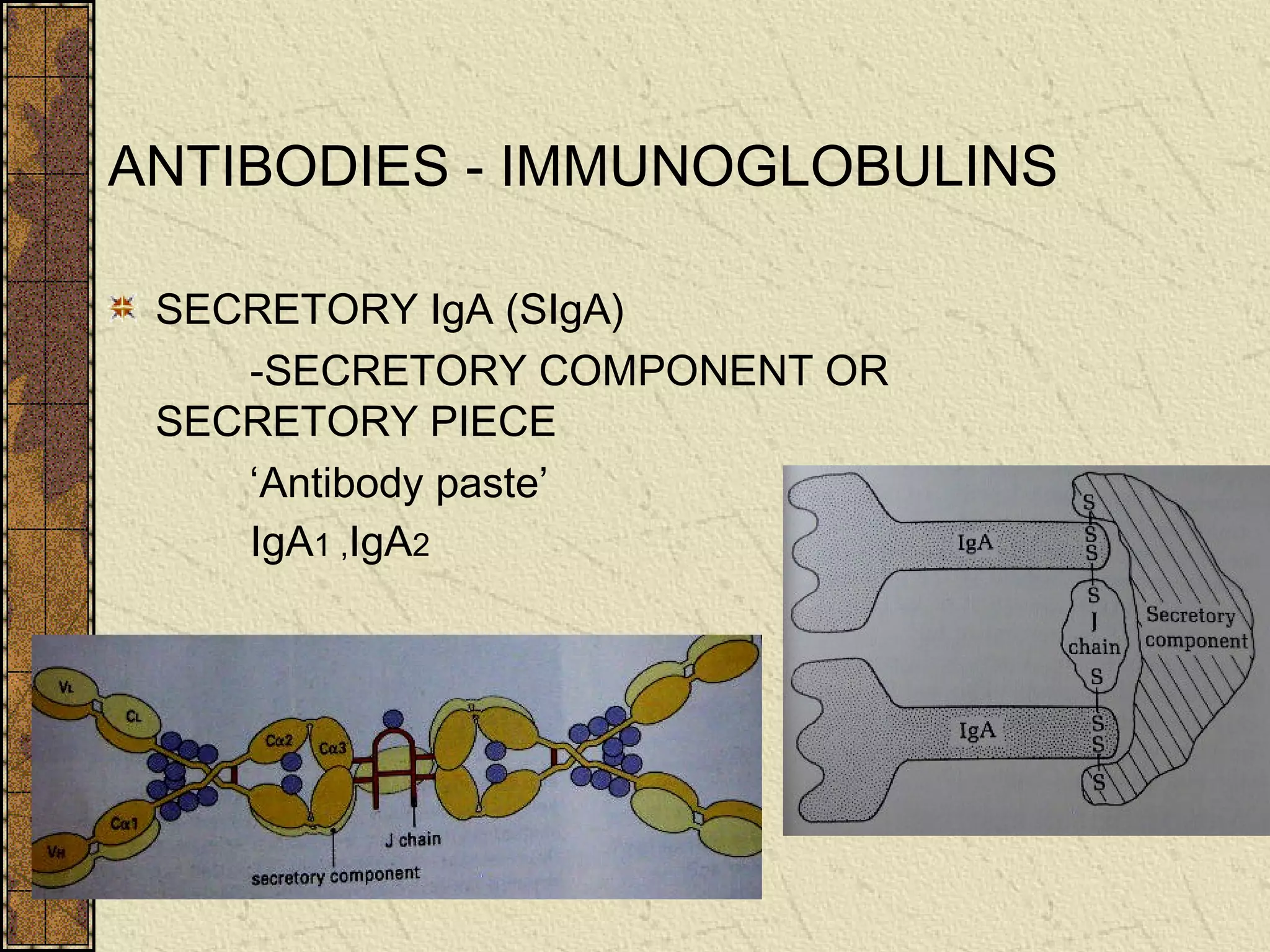
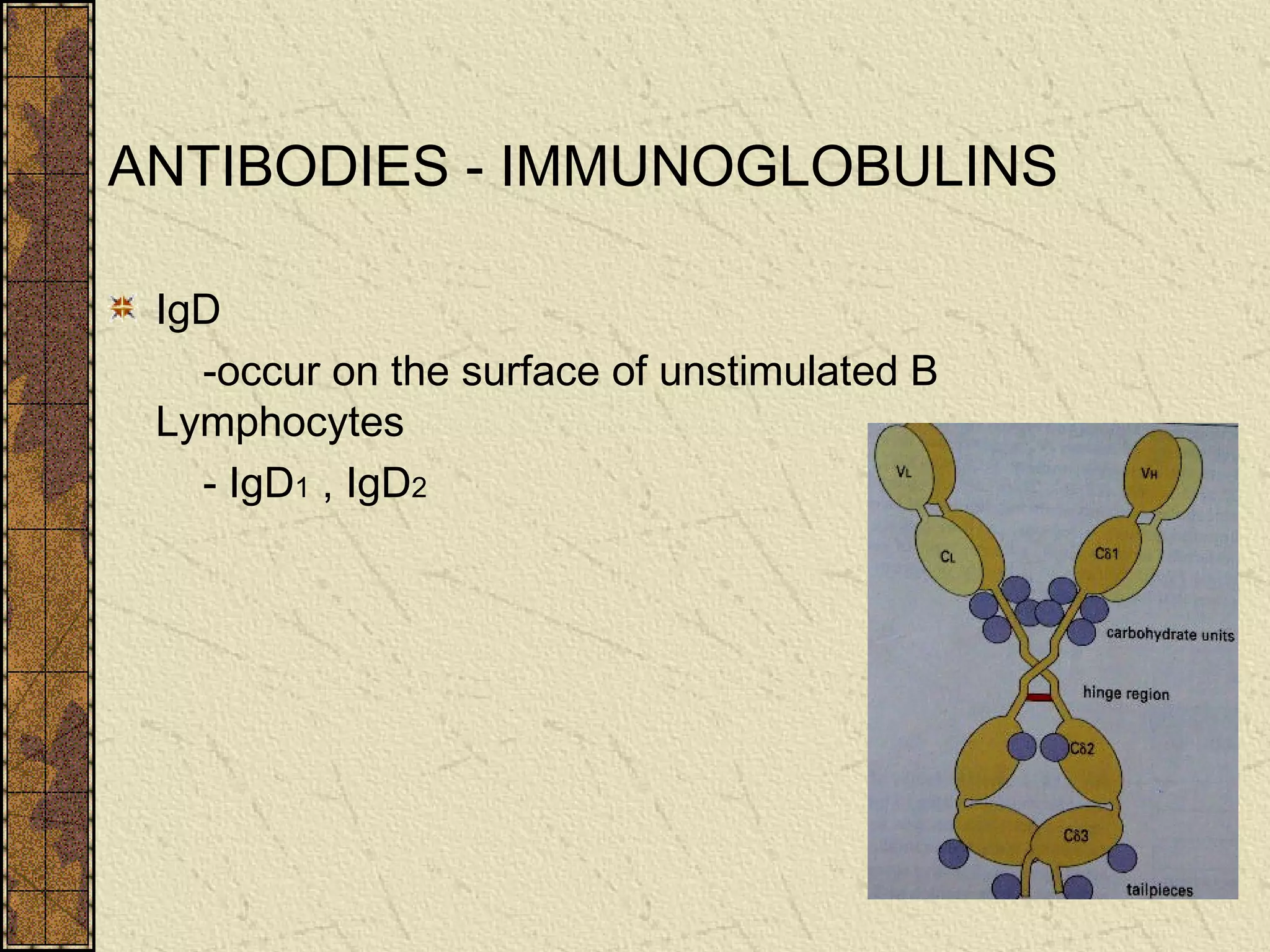
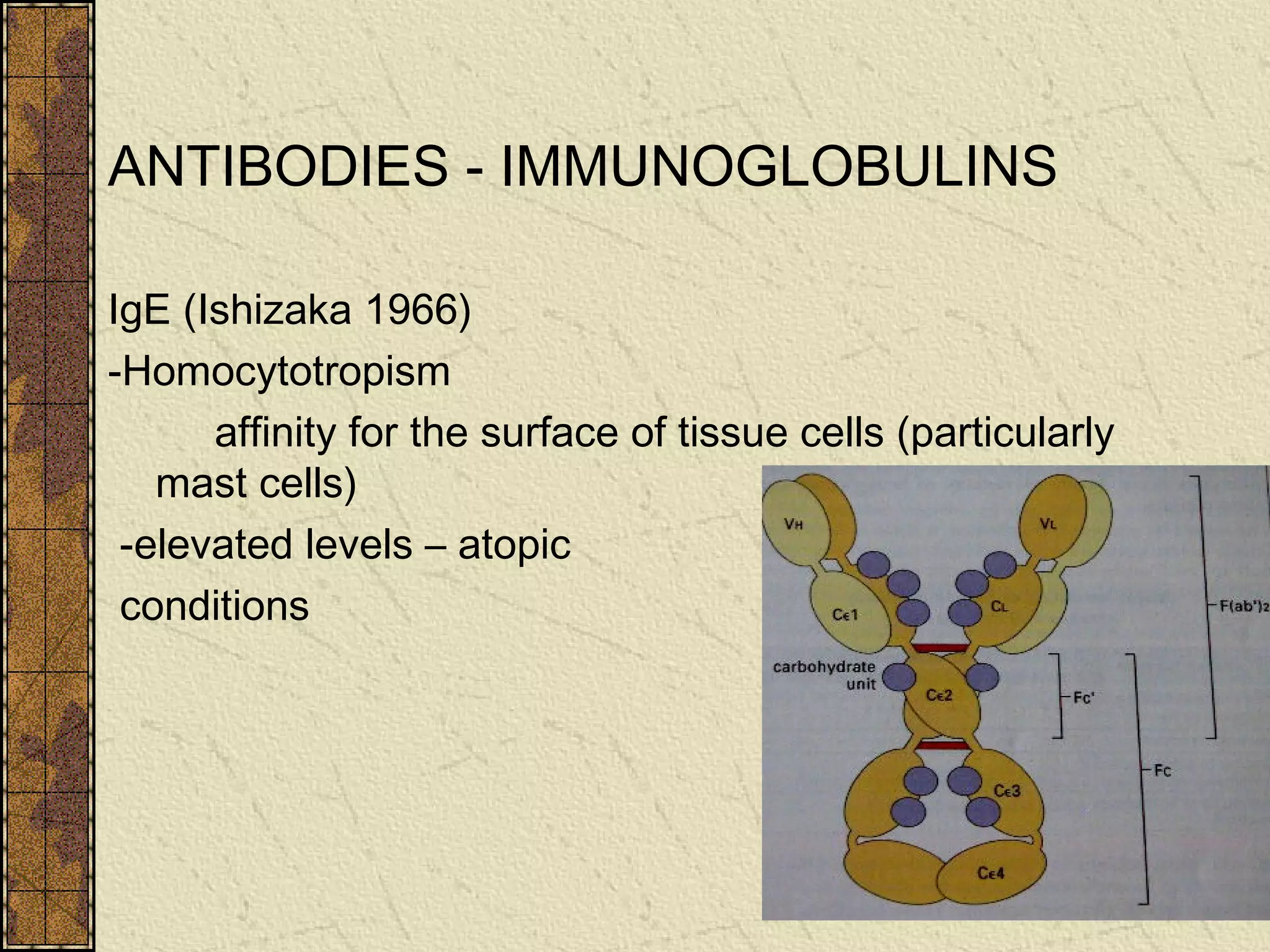
Definition of antigens, antibody types, and structure of immunoglobulins, highlighting their functional importance.
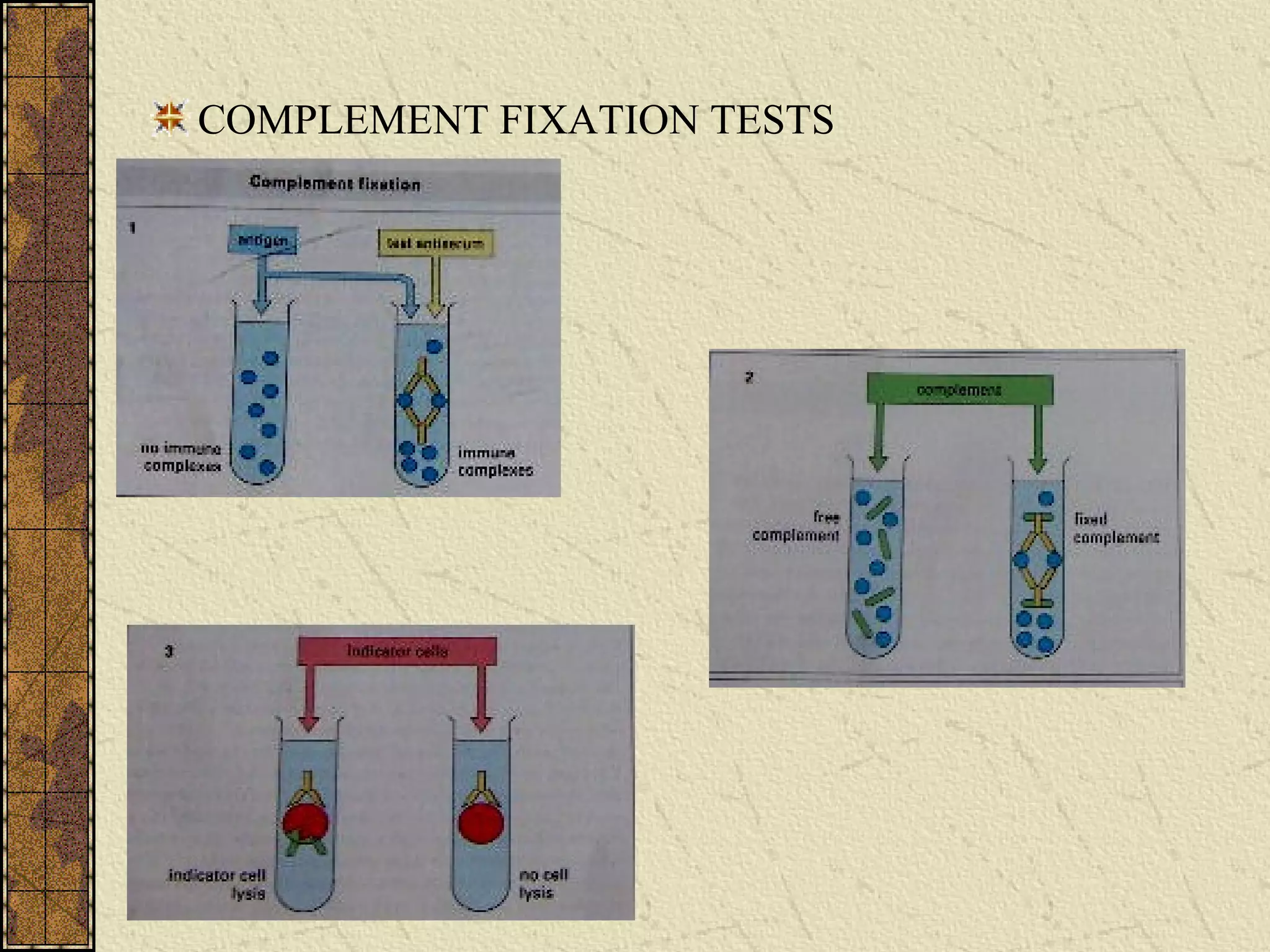
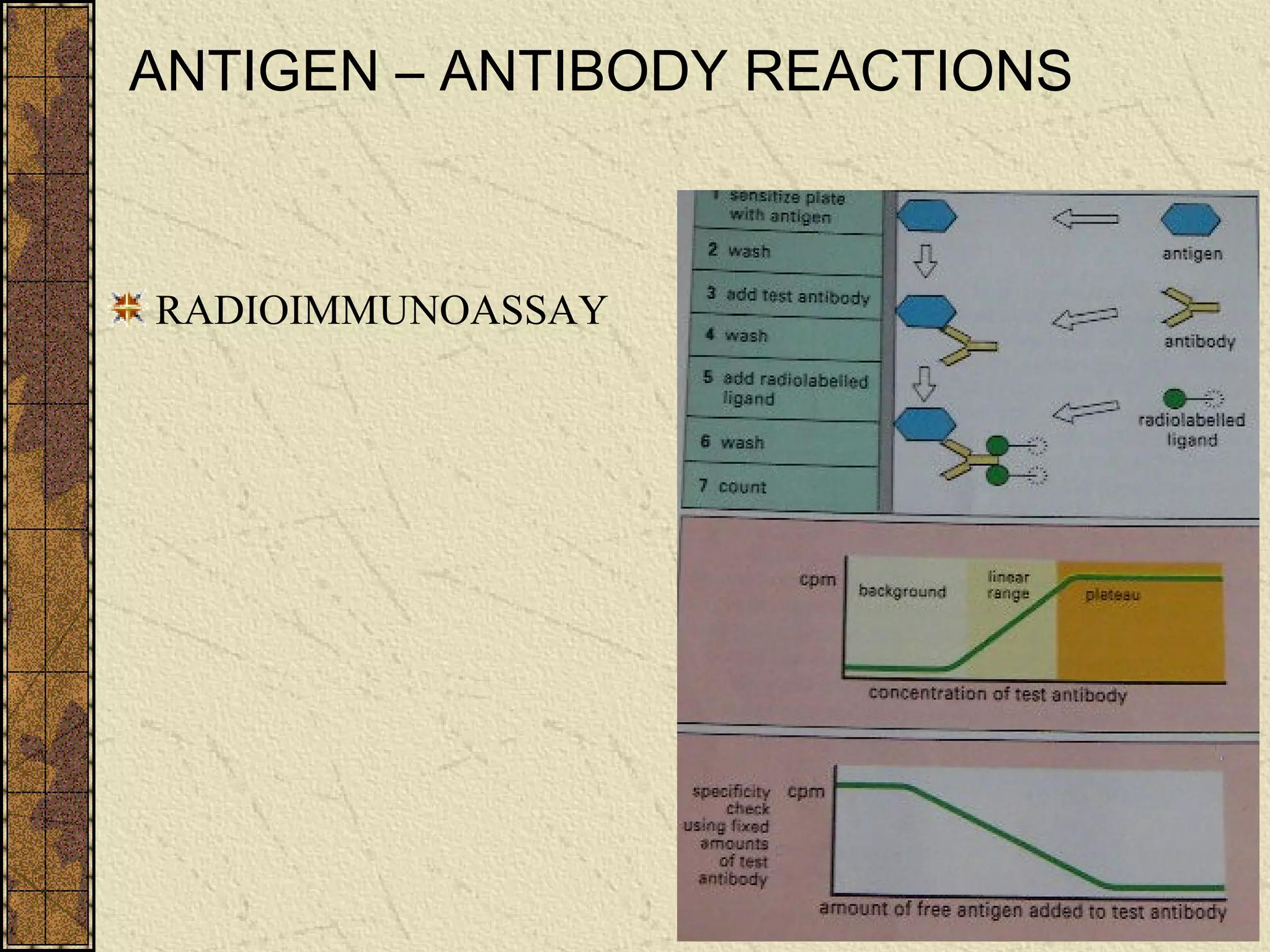
Stages and features of antigen-antibody interactions including precipitations and agglutination applications.
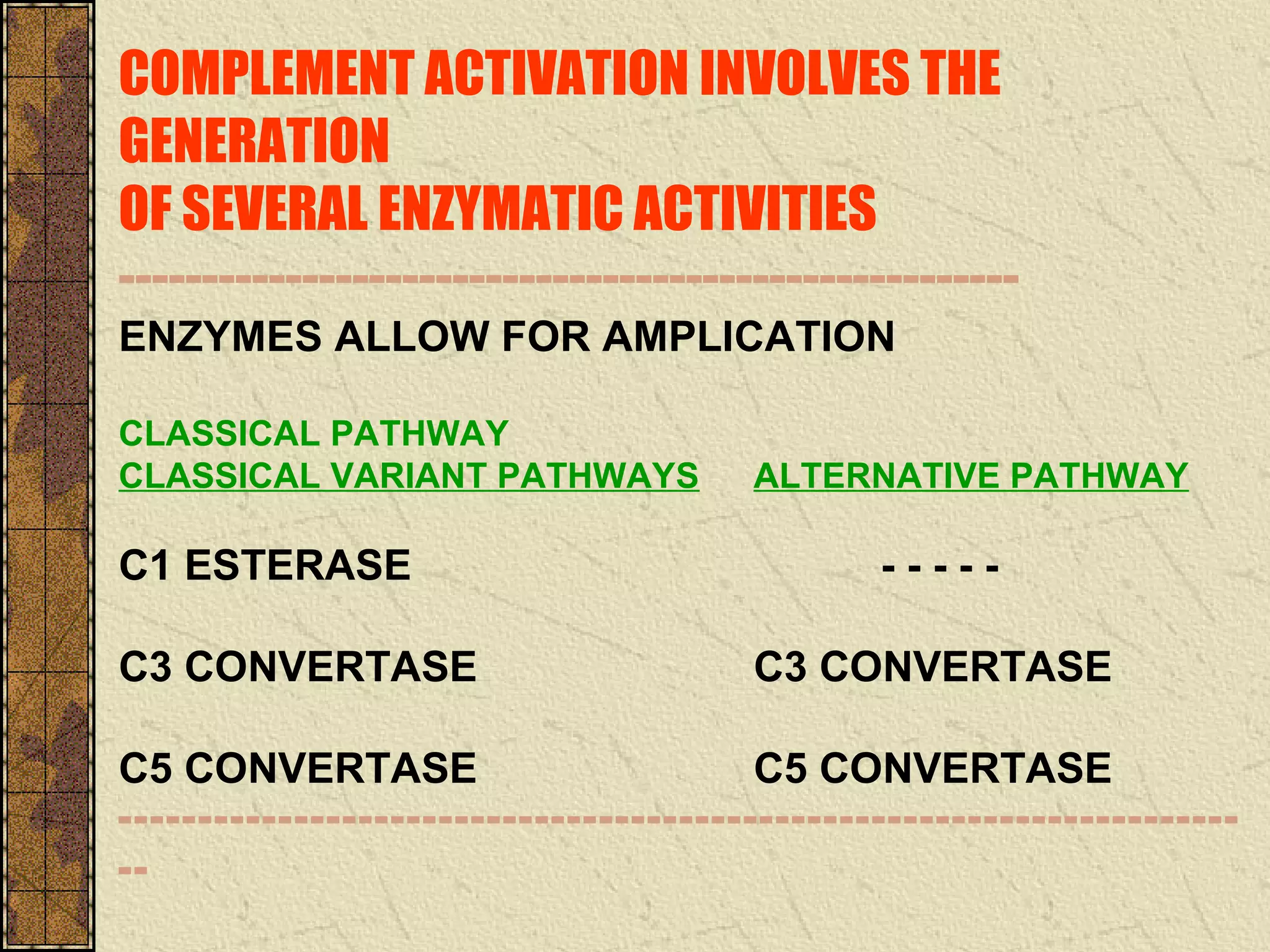
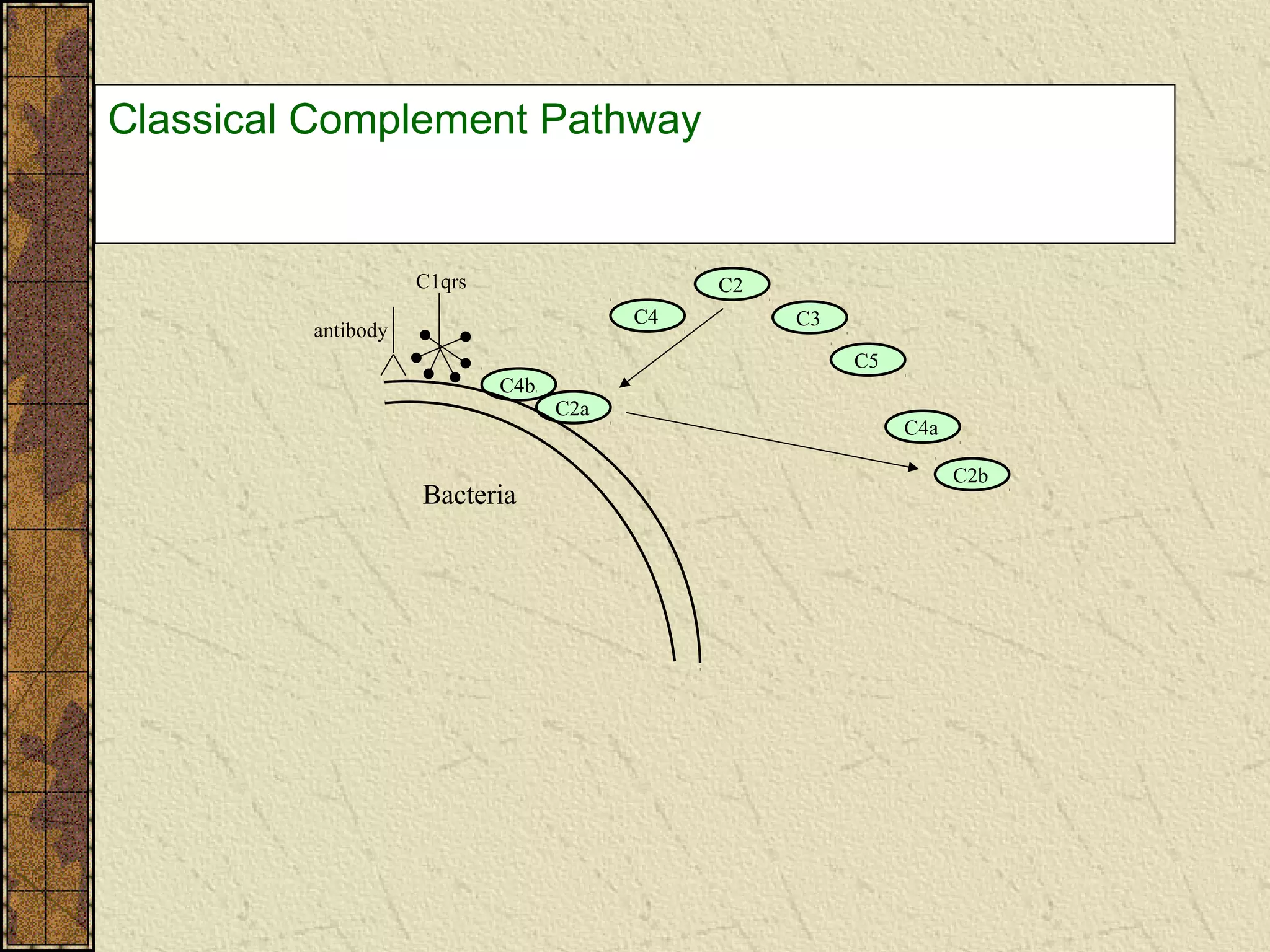
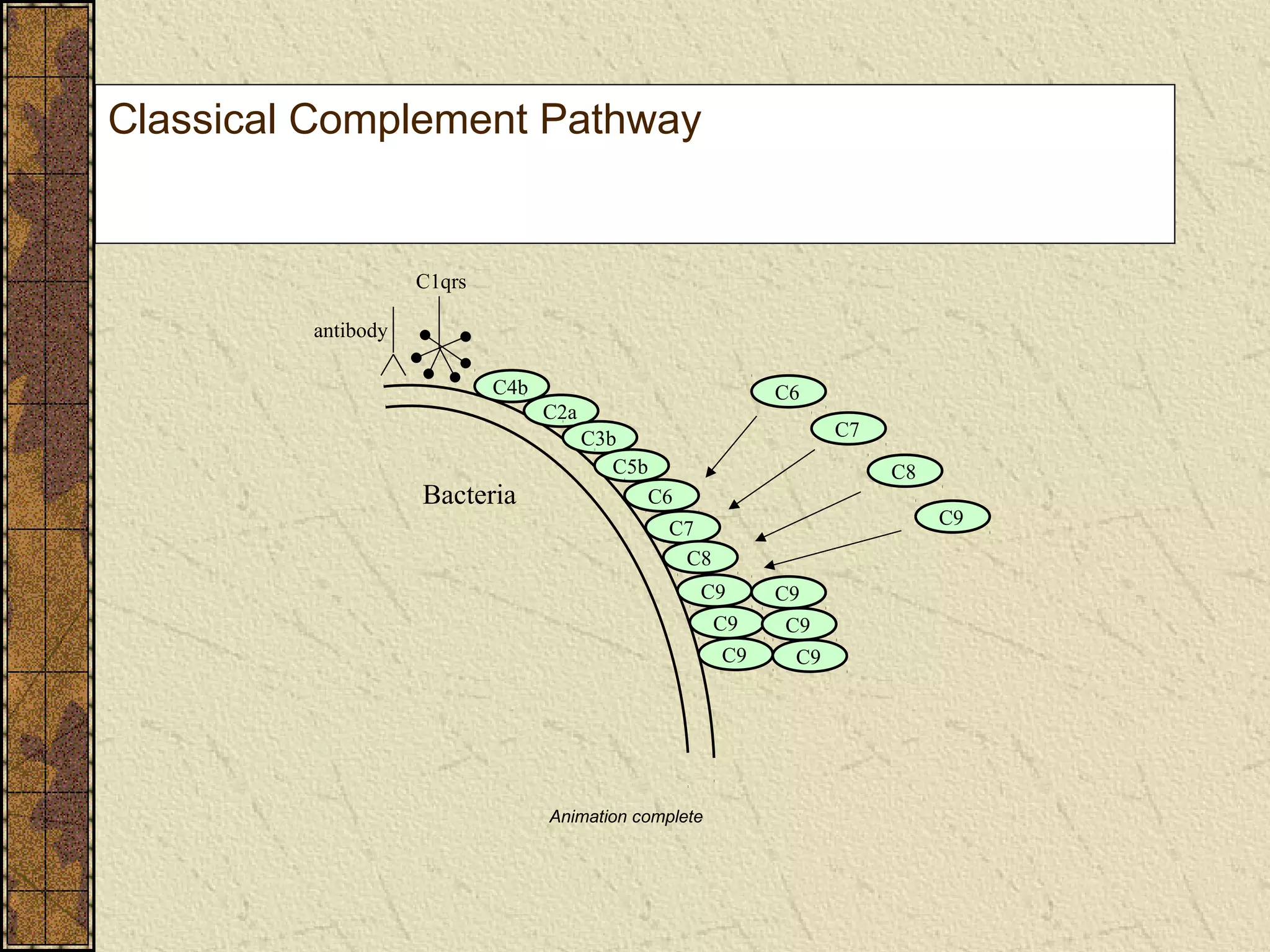
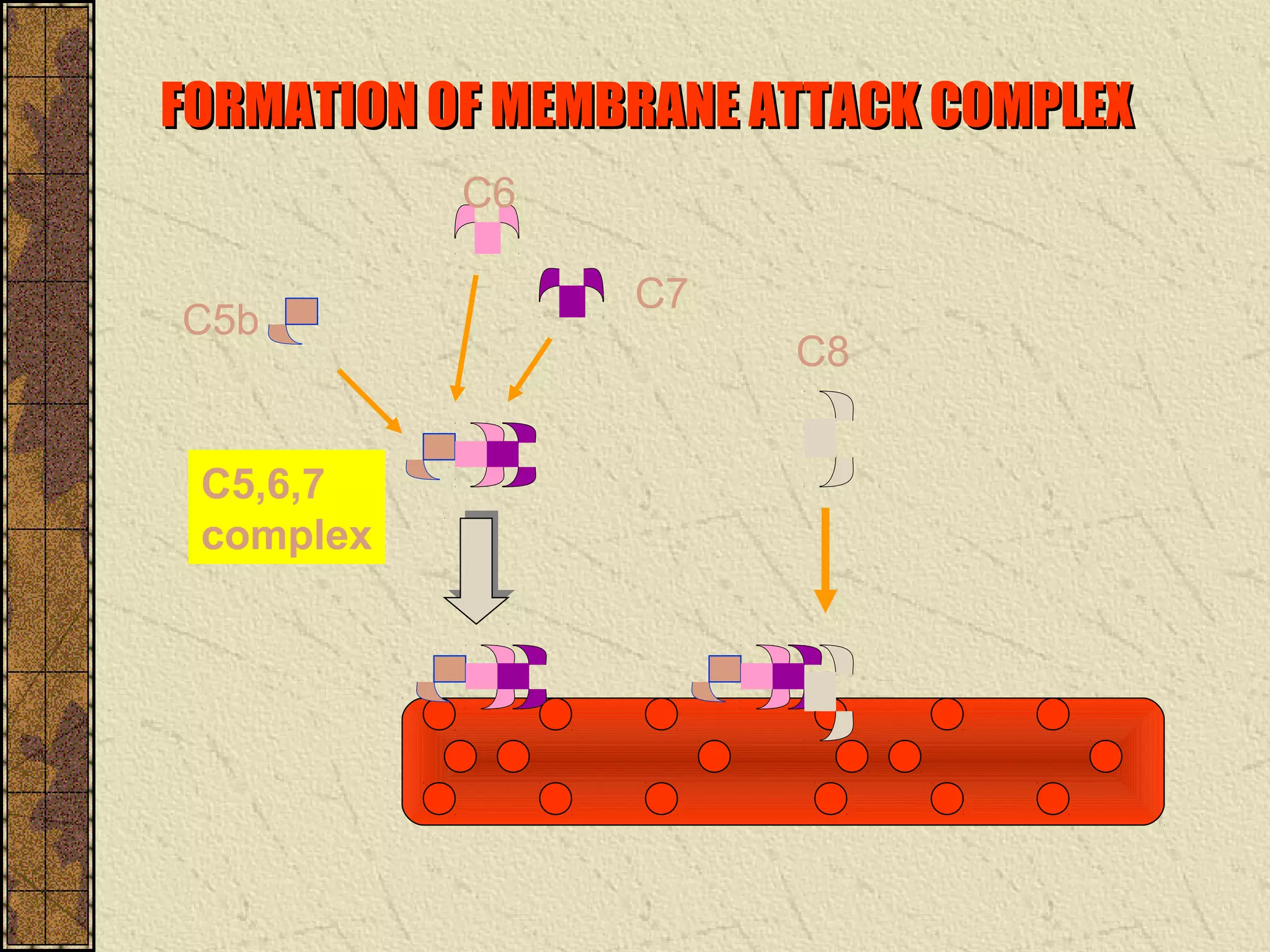
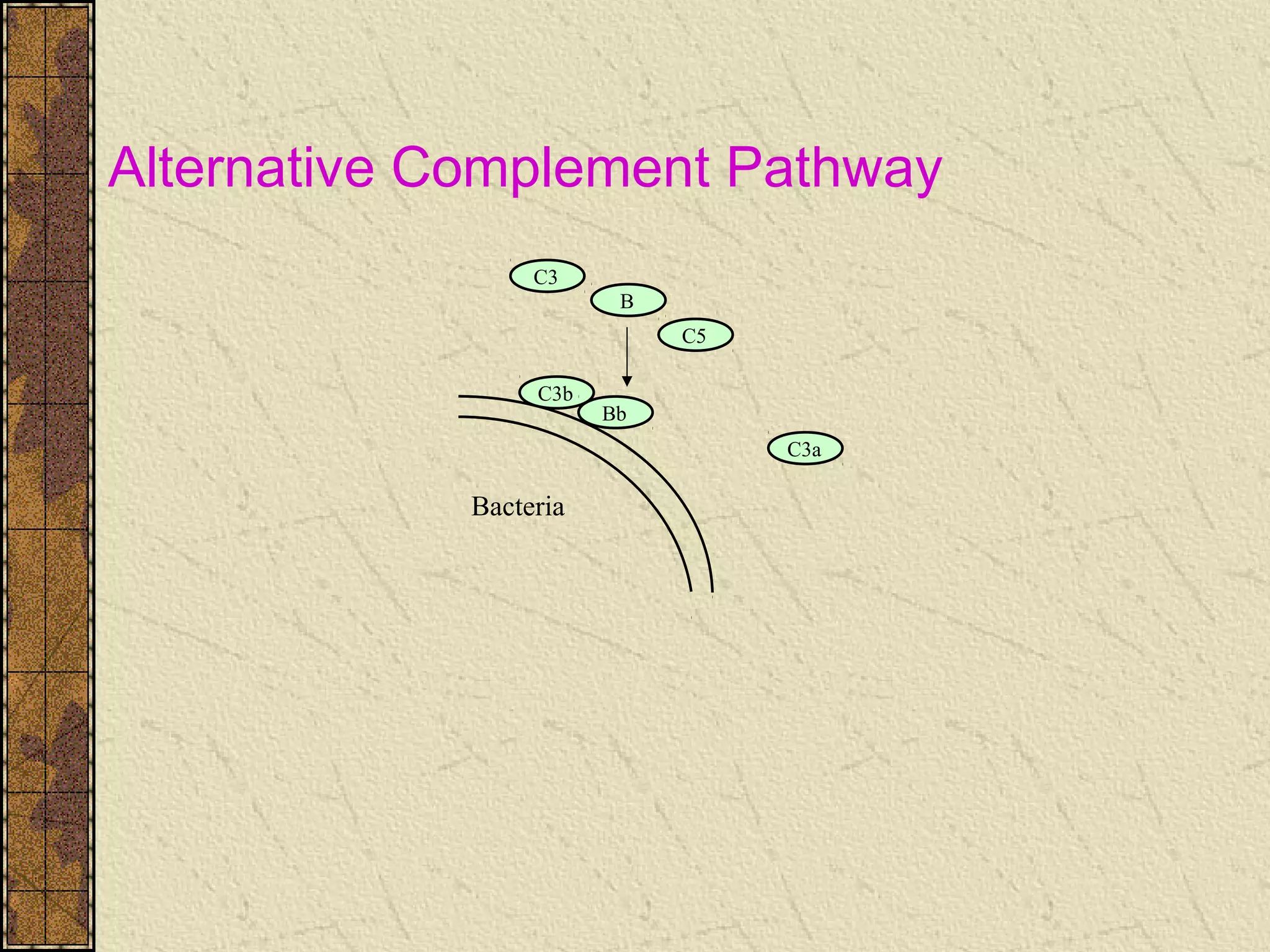
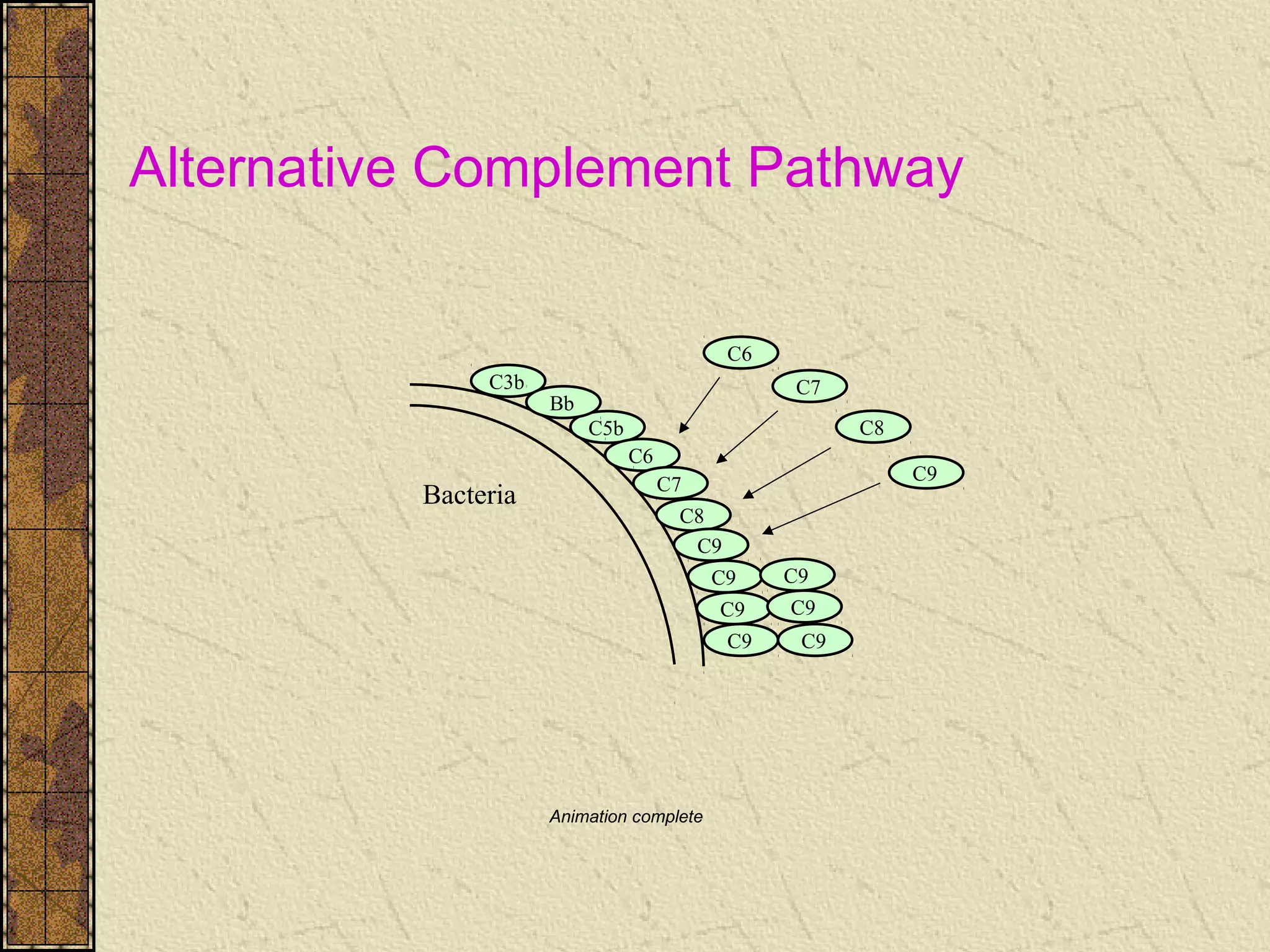
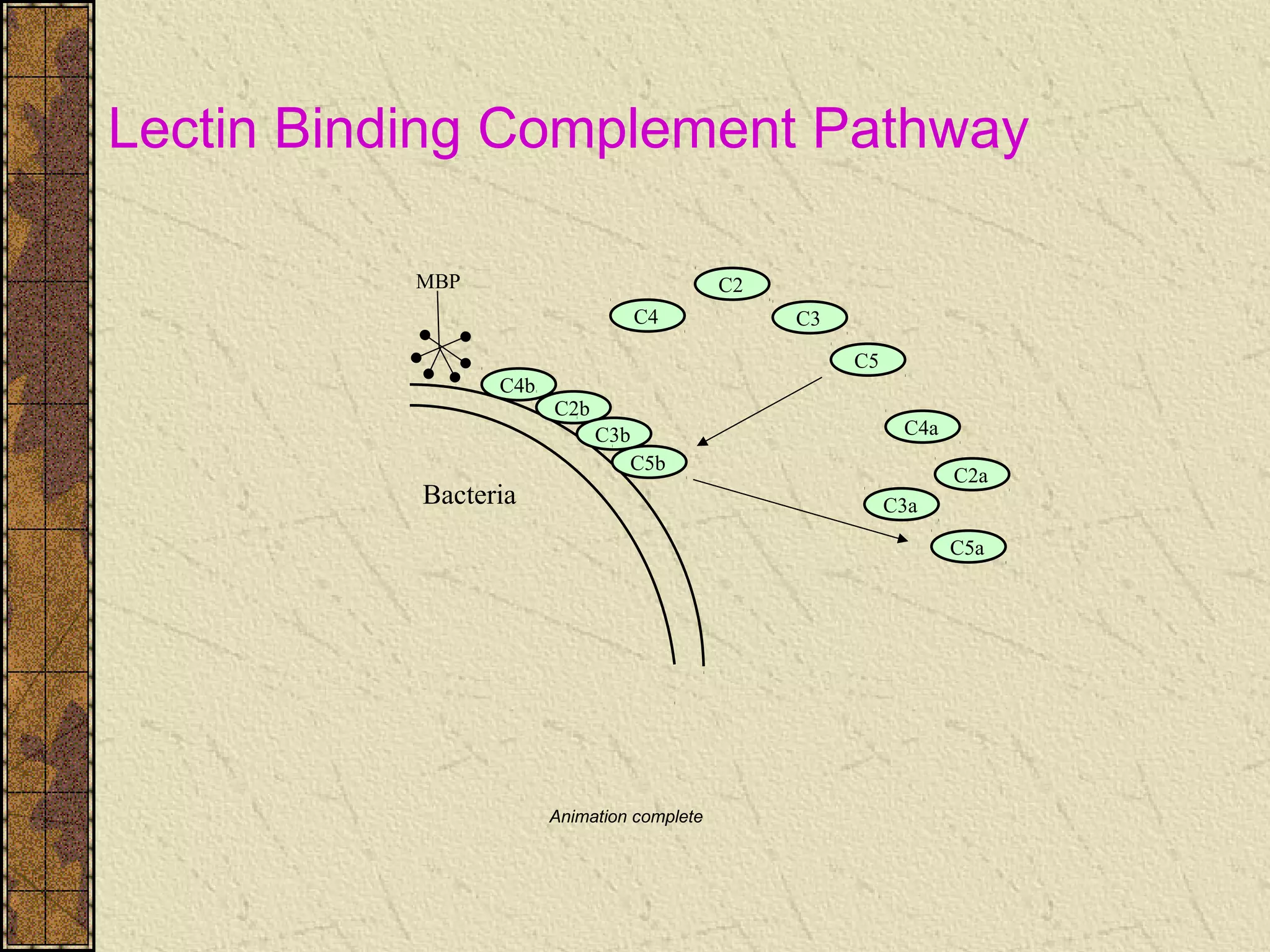
The complement system's structure, activation, and regulatory mechanisms, including various pathways.
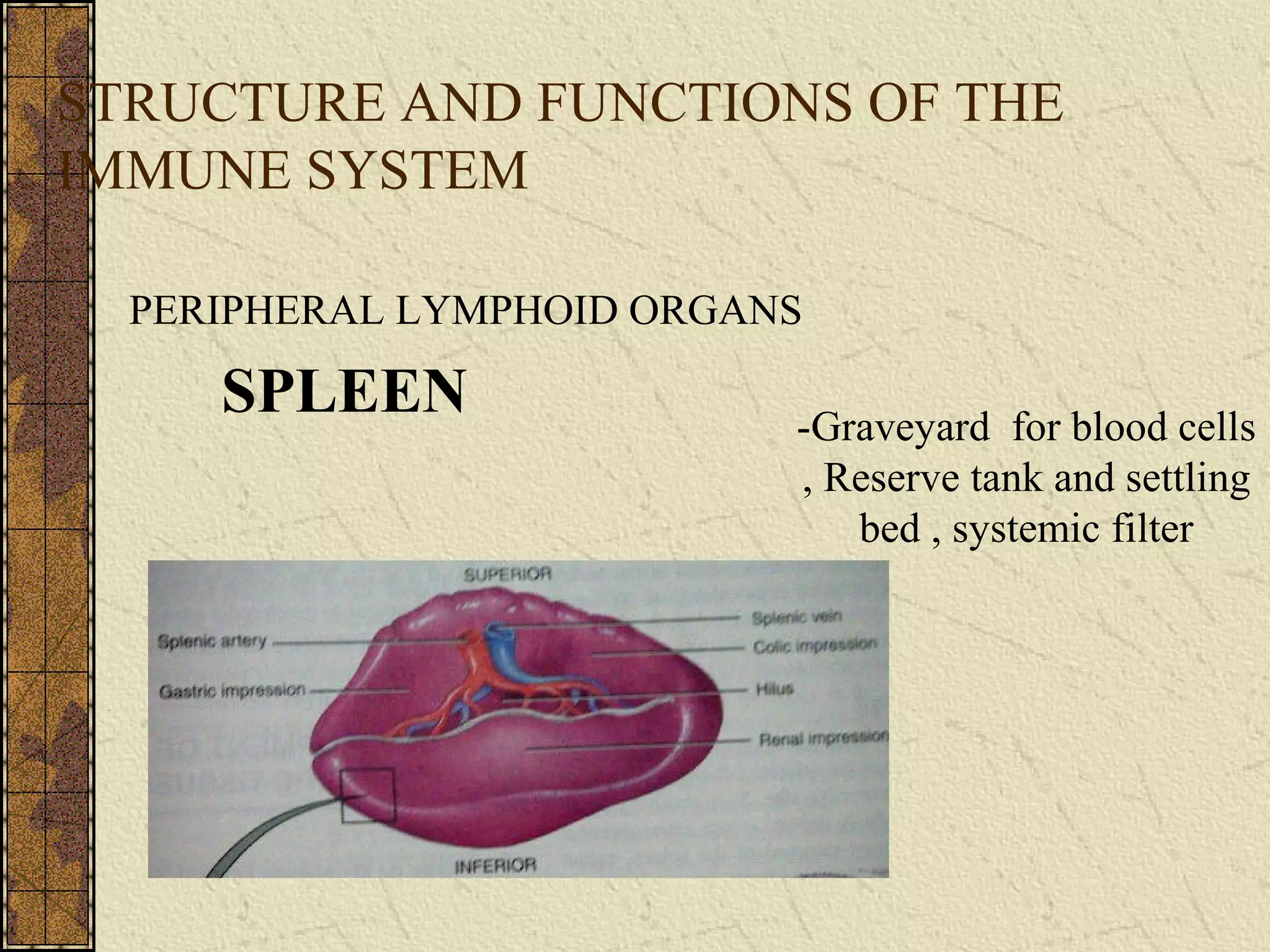
Overview of lymphoid organs, types of lymphocytes, and their roles in the immune response.
Characteristics and functions of phagocytic cells and their importance in innate immunity.
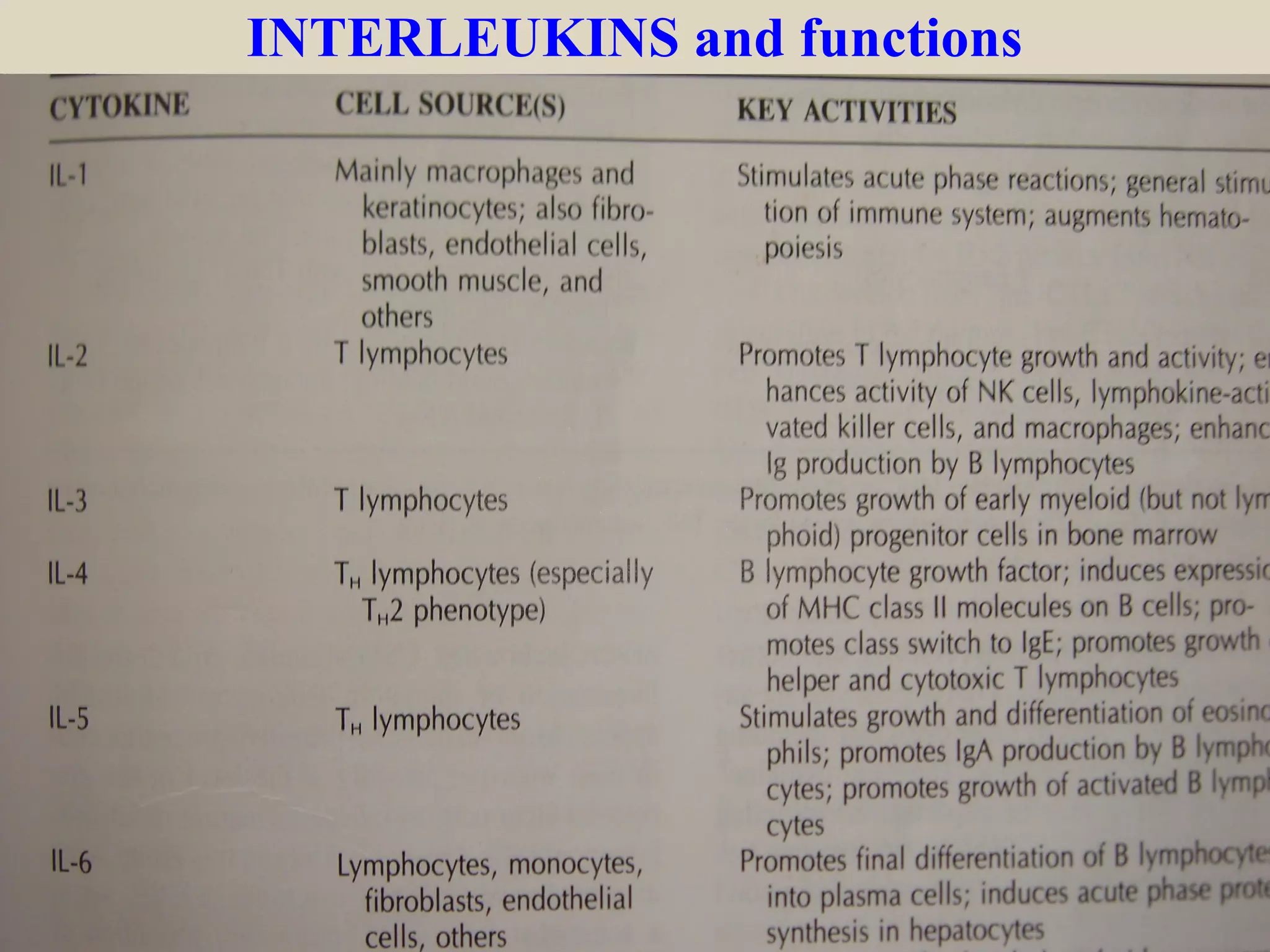
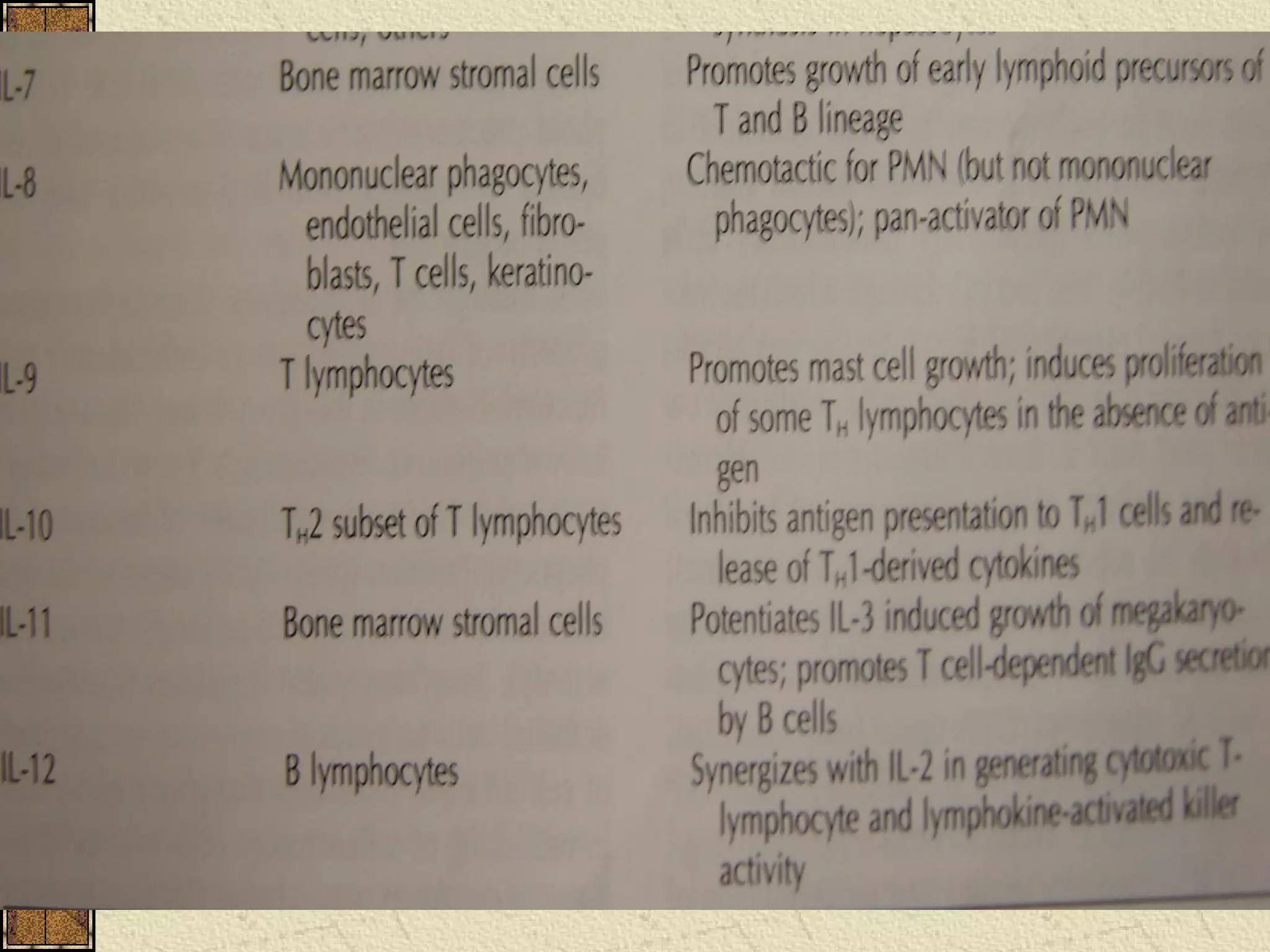
Introduction to cytokines, their types, and roles in mediating immune responses and inflammation.
Primary and secondary immunodeficiencies, their causes, and examples of disorders affecting immunity.
Description of autoimmune diseases, mechanisms like neoantigens, and features and classifications of autoimmune conditions.
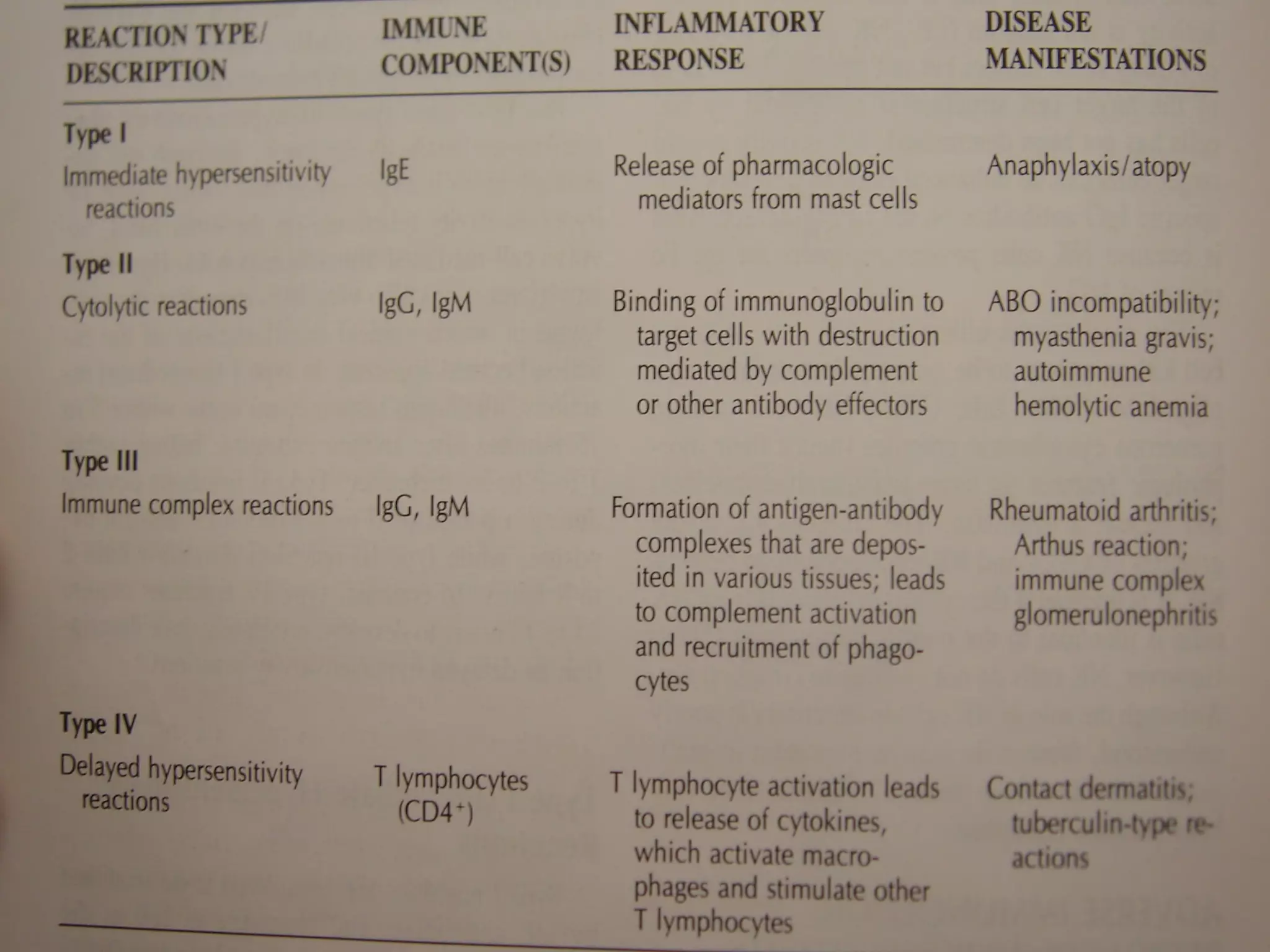
Definition and classification of hypersensitivity reactions including types of immune system responses that cause injury.Overview of salivary components in innate immunity, their roles in antibacterial action and overall oral health.
Emerging vaccine strategies for oral diseases, including methods of antigen administration and immune stimulation.
Immunological responses during periodontal disease progression and systemic effects including inflammation.
Summary of the immune system's protective roles and the importance of immunological knowledge in clinical practice.
List of key textbooks and research articles for continued learning on immunology and oral health.


































































































