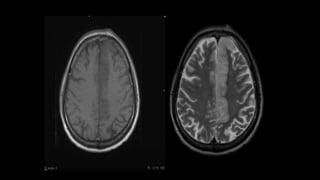
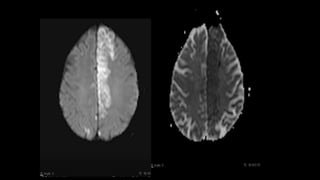
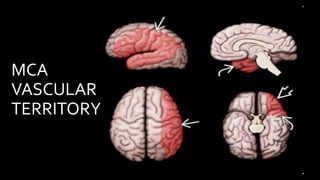
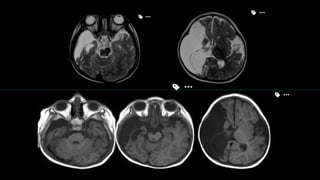
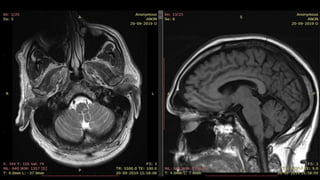
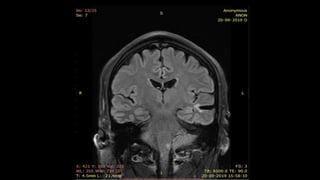
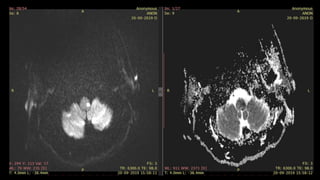
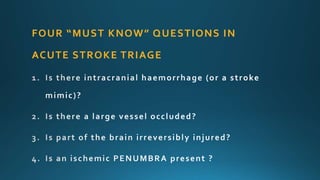
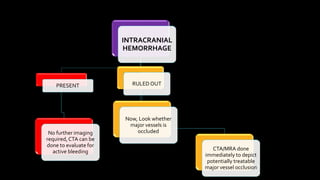
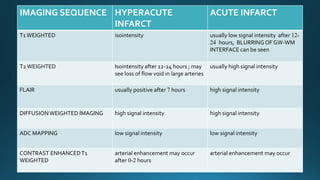
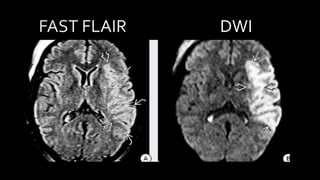
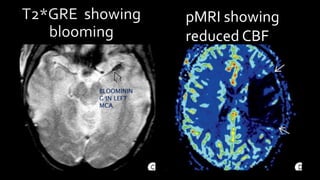
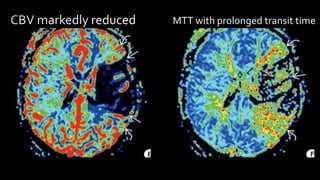
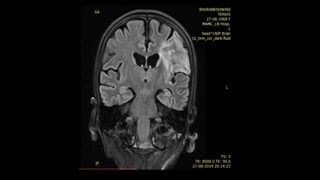
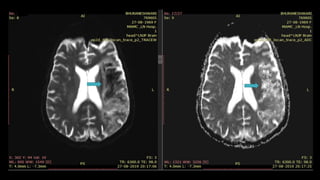
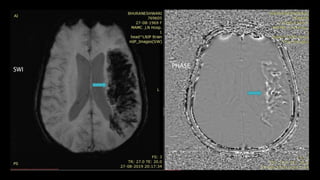
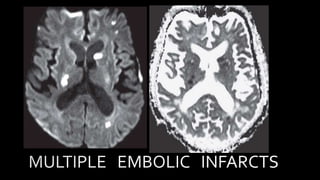
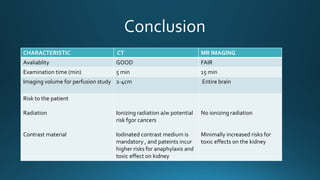
The document discusses the role of MR imaging in the diagnosis and management of stroke, highlighting the differences between ischemic and hemorrhagic strokes and the importance of imaging in triaging treatment options. It outlines the various neuroimaging techniques, their timeframes for stroke detection, and the critical information needed to determine the presence of reversible ischemic penumbra and the extent of infarction. Additionally, it emphasizes the advantages of MRI over CT in detecting hyperacute ischemic changes and the implications of imaging findings for treatment decisions.