Hyphema, Basic Information
•Download as PPTX, PDF•
15 likes•7,278 views

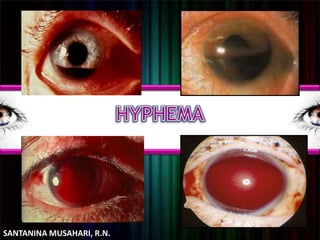
This document discusses traumatic hyphema, which is bleeding into the anterior chamber of the eye following an eye injury. It can be caused by blunt trauma, surgery, or spontaneously from conditions like tumors or blood clotting issues. Symptoms include blurred vision, pain and photophobia. Treatment involves protecting the eye, preventing further bleeding with medications, and sometimes surgically removing blood if pressure rises too high. Goals are to prevent secondary glaucoma and damage to vision.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hyphema, Basic Information
Similar to Hyphema, Basic Information (20)
Recently uploaded
Recently uploaded (20)
Hyphema, Basic Information
- 2. — Frank bleeding into the anterior chamber following contusion of the globe. —Disruption of blood vessels in the iris or ciliary body —This blood usually does not clot —w/ bed rest, a red fluid meniscus is form
- 3. • separates the cornea from the lens, both of which work together to focus light onto the retina. The anterior chamber is full of clear fluid called aqueous humor, which is important for the health of the cornea.
- 4. Blunt Trauma Intraocular surgery Lacerating trauma Penetrating and perforating injury It also occurs spontaneously w/o any trauma, usually neovascularization, tumor of eye (Retinoblastoma), uveitis or vascular anomalies Use of medicine which impair blood clotting such as aspirin and analagesic
- 5. • Traumatic Hyphema occurs most often from a tear in the anterior surface of the ciliary body, with resultant disruption of the major arterial circle of the iris, arterial branches to the ciliary body or vein coursing between the ciliary body and episcleral venous plexus
- 6. • There are 2 suggested mechanism of hyphema formation – 1. direct contusive force cause mechanical tearing of blood vasculature of iris and or angle – 2. Concussive trauma creating rapidly rising intravascular pressure with in the vessels resulting in rupture of vessels
- 8. Grade Size of Hyphema 0 I No layered blood circulating red blood cells only Less than 1/3 II 1/3 to 1/2 III 1/2 to less than total IV Total
- 10. • Injured eye should be protected with a shield for 1 to 2 weeks after injury. • Systemic Aminocaproic acid ( Amicar [100mg/kg of body weight every 4 hrs orally for 5 days], an inhibitor of fibrinolysis, may prevent early clot retraction within injured intraocular vessel and reduced the possibility of secondary hemorhhage. • Spontaneous Recovery usually occur if the AC in not entirely filled w/ blood
- 11. • Minor rises in IOP – Treated w/ topical timolol and systemic acetazolamide. • Surgical Indication: – Inc. IOP of >50 mmHg – Persistently (5 to 7 days) high pressure – Early blood staining of the cornea • Simple removal of small amount of aqueous humour (Anterior Chamber Paracentesis) or Irrigation of AC may be effective
- 12. – Clots should never be removed by means of forceps due to difficulty distinguishing clot from iris. – Vitrectomy irrigator aspirator maybe used to aspirated the blood. • Inserted through the corneoscleral limbus • Care must be taken not to injure the endothelium, iris or lens. • General anesthesia is usually desirable due to difficulty anesthetizing the congested eye • If IOC is increase, give IV mannitol to reduced the pressure before incision into AC
- 13. • Blood in the anterior chamber is not by it self necessarily harmful. However, if the quantities are sufficient it may obstruct the outflow of Aqueous humour, resulting In Glaucoma • The original hyphema, w/c is often relatively minute and absorbed in 2 to 3 days, may be followed by more severe bleeding 3 to 5 days after the original injury. A secondary Glaucoma may occur immediately.
- 14. • Secondary glaucoma – May cause optic atrophy, corneal blood staining and adhesion between the peripheral iris and anterior chamber angle ( peripheral anterior synechiae. – When anterior chamber is filled w/ blood, prolong secondary glaucoma causes staining of the cornea. • Corneal stroma is infiltrated by hemosiderin, w/c causes deep yellowish green opacity of the cornea
- 15. • Aspirin and related analgesics w/c impair blood clotting should not be used to relieve pain – Acetaminophen may be substituted.