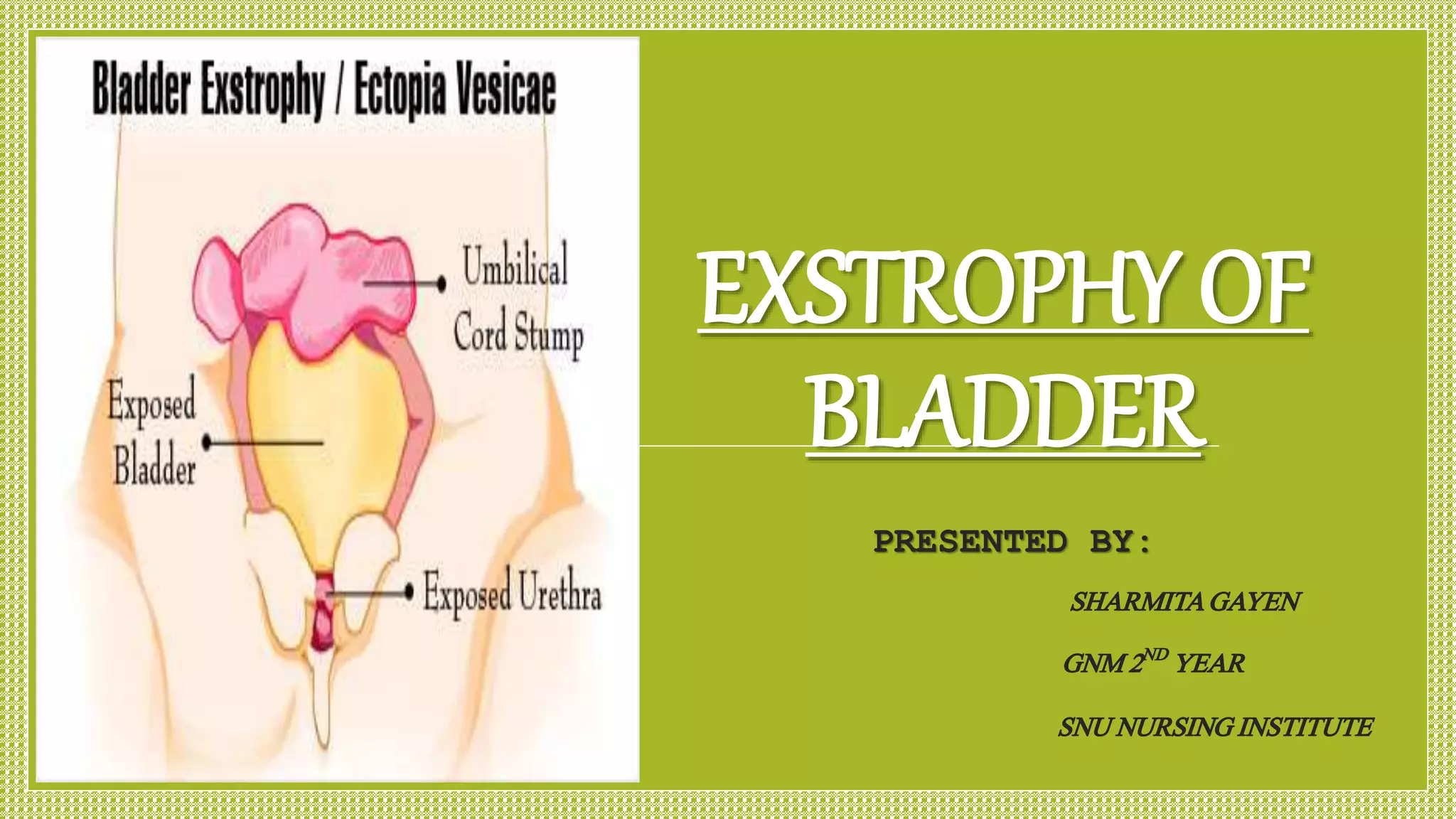
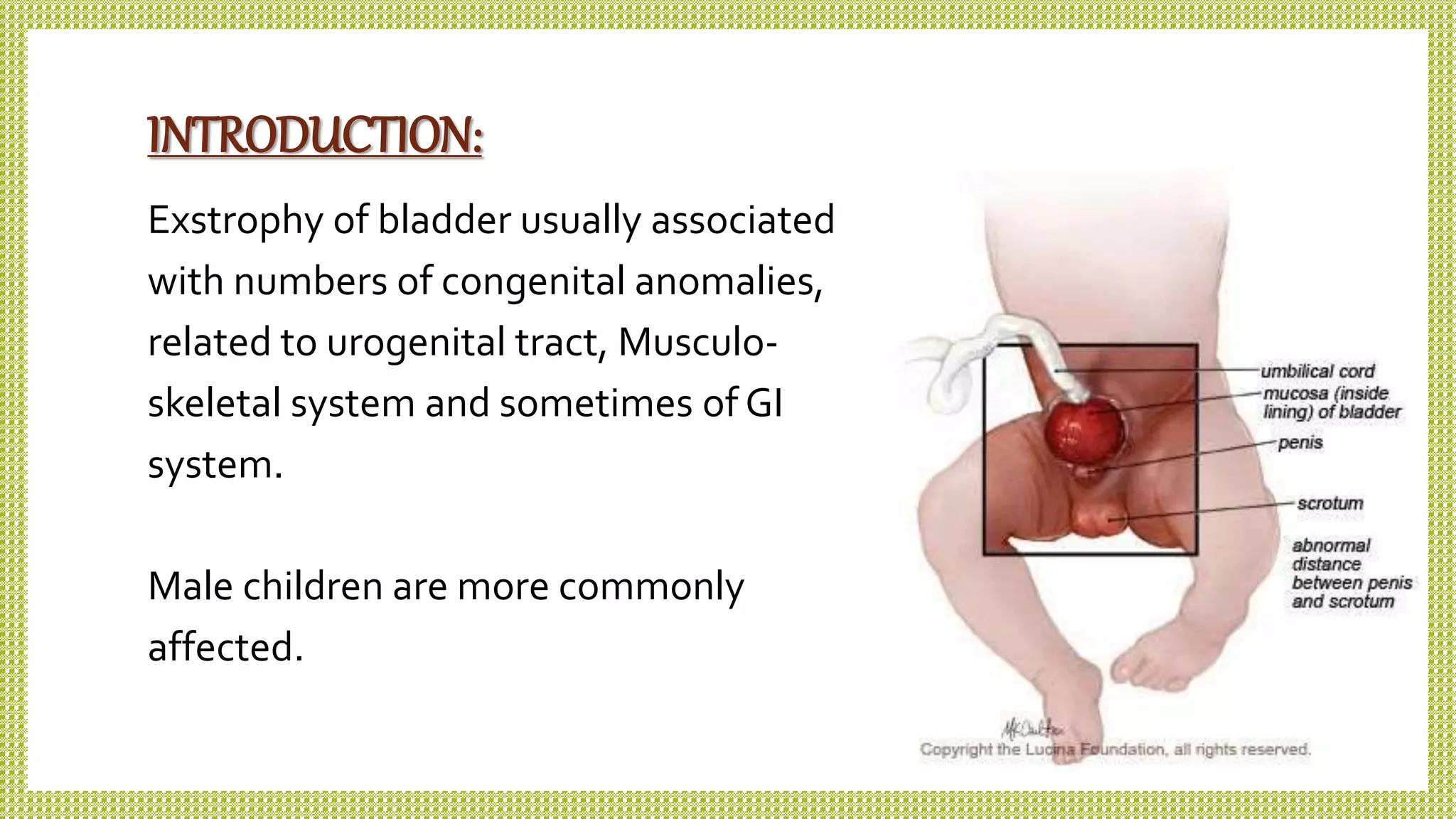
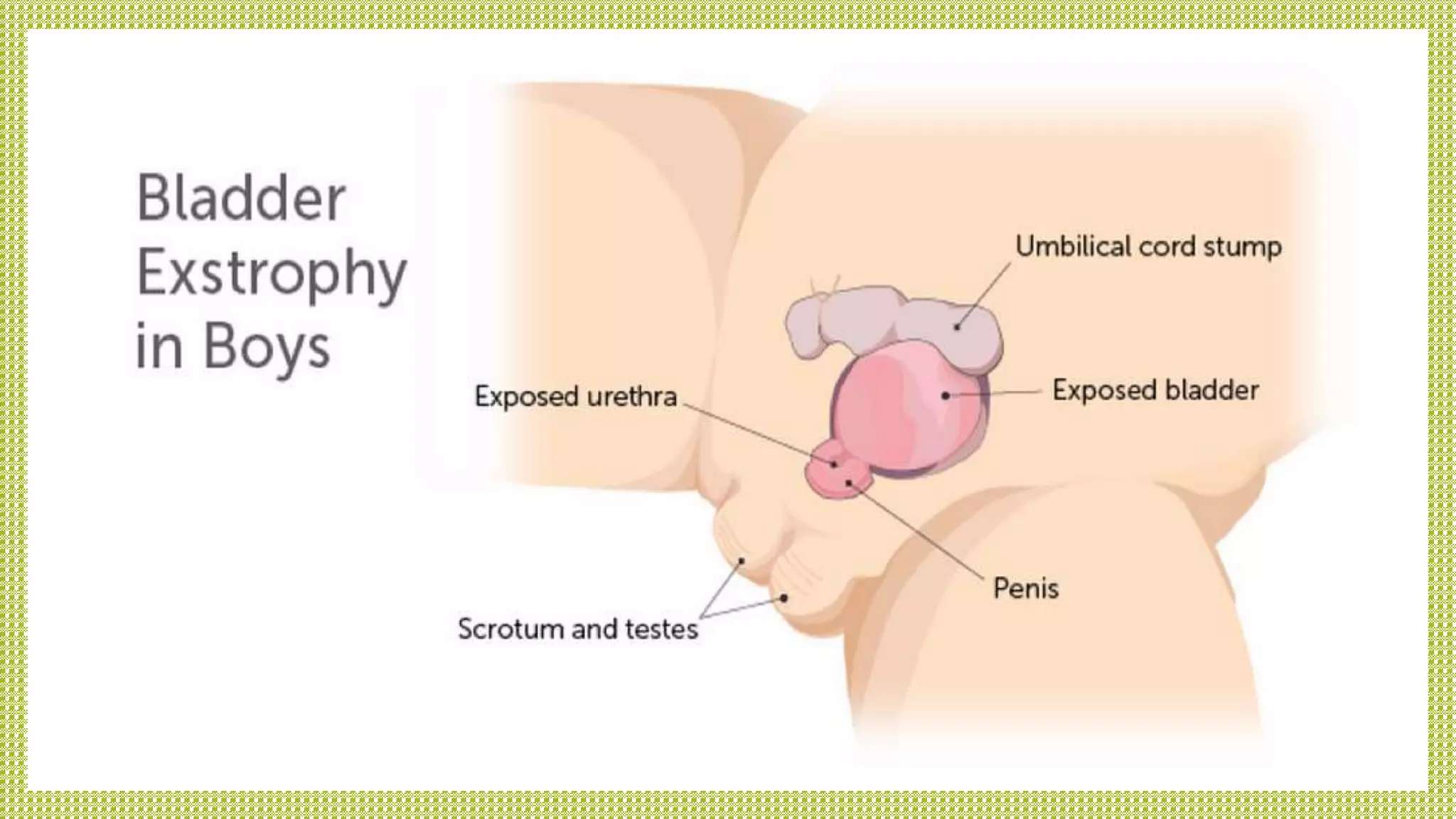
Exstrophy of bladder is a congenital malformation characterized by the exposure of the bladder due to improper formation of the abdominal wall, predominantly affecting males. The condition, which affects 1 in 10,000 to 1 in 50,000 live births, requires thorough medical and surgical management, including repair surgeries and supportive nursing care to prevent infections and maintain hygiene. Prognosis post-surgery is generally positive, with about 80% of patients expected to achieve urinary continence, though long-term complications may persist.