Downloaded 1,898 times


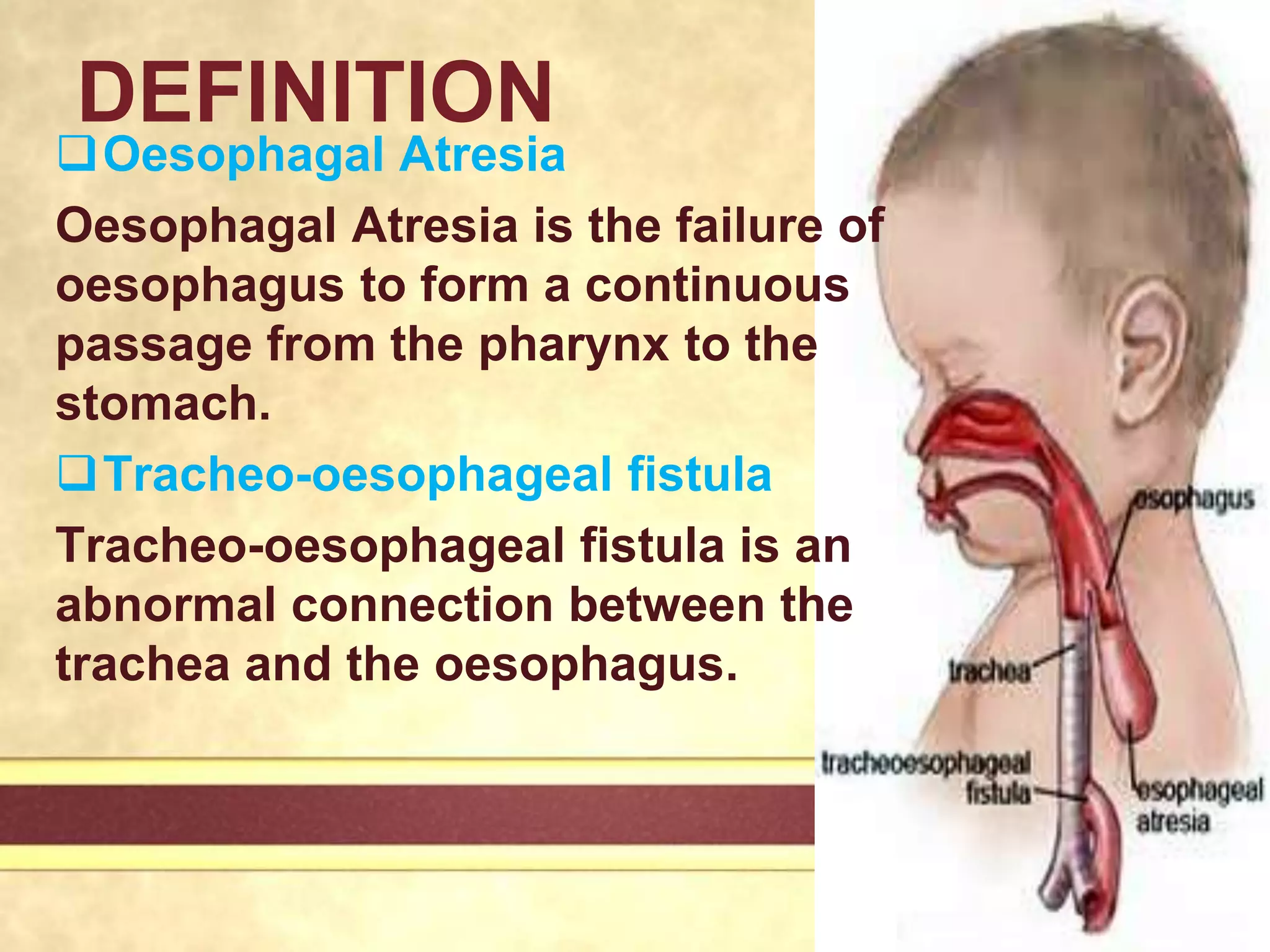




















Tracheo-oesophageal fistula and oesophagal atresia are birth defects where the esophagus does not form properly, either failing to connect to the stomach or connecting abnormally to the trachea. They occur in about 1 in 3500 births. Surgical intervention is required to divide any abnormal connections or perform anastomosis to reconnect the esophagus. Nursing care focuses on preventing aspiration, maintaining nutrition via feeding tubes, and managing pain and comfort after surgery. Complications can include tracheomalacia, anastomotic leaks, strictures, and reflux.

























































