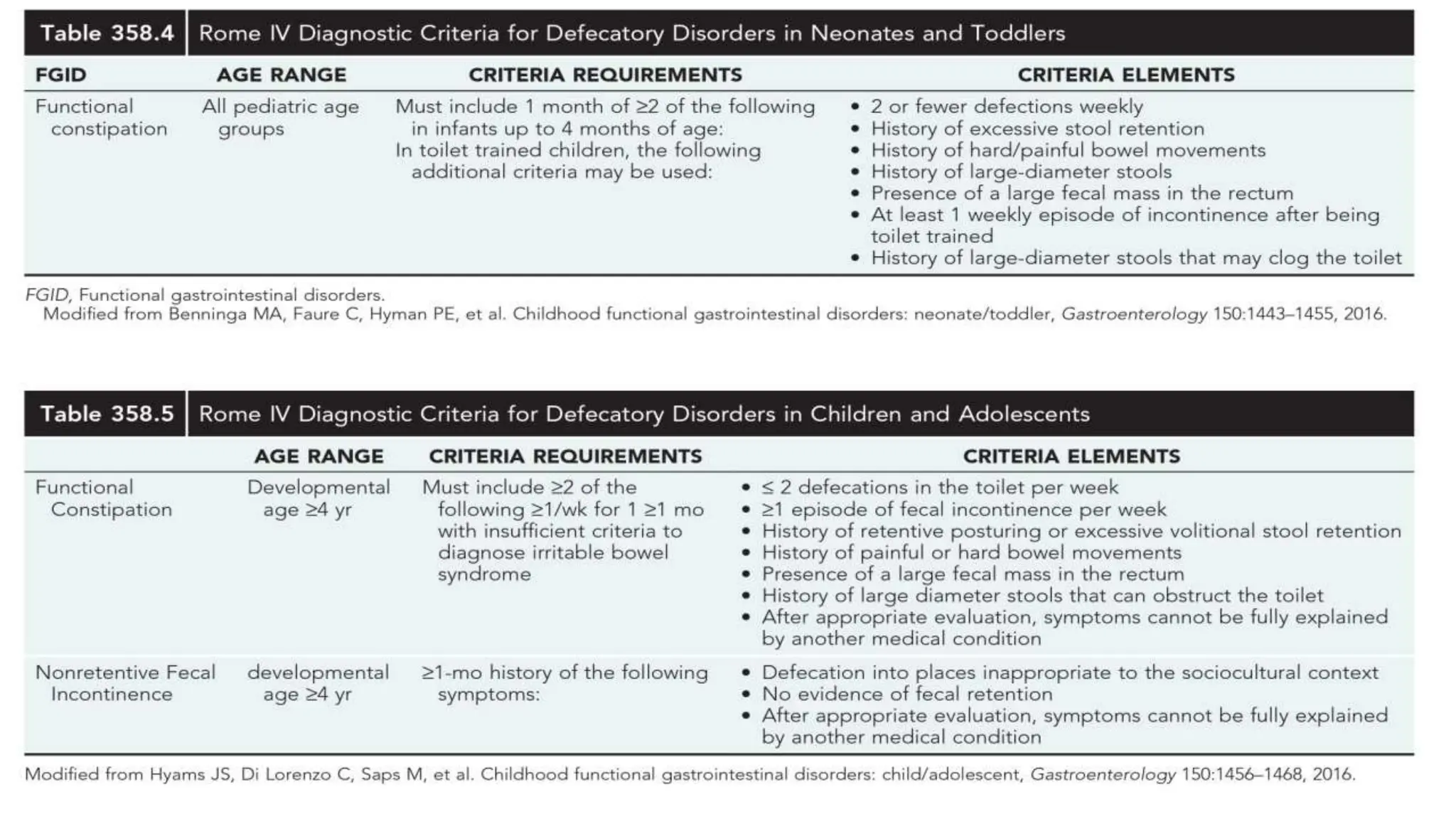
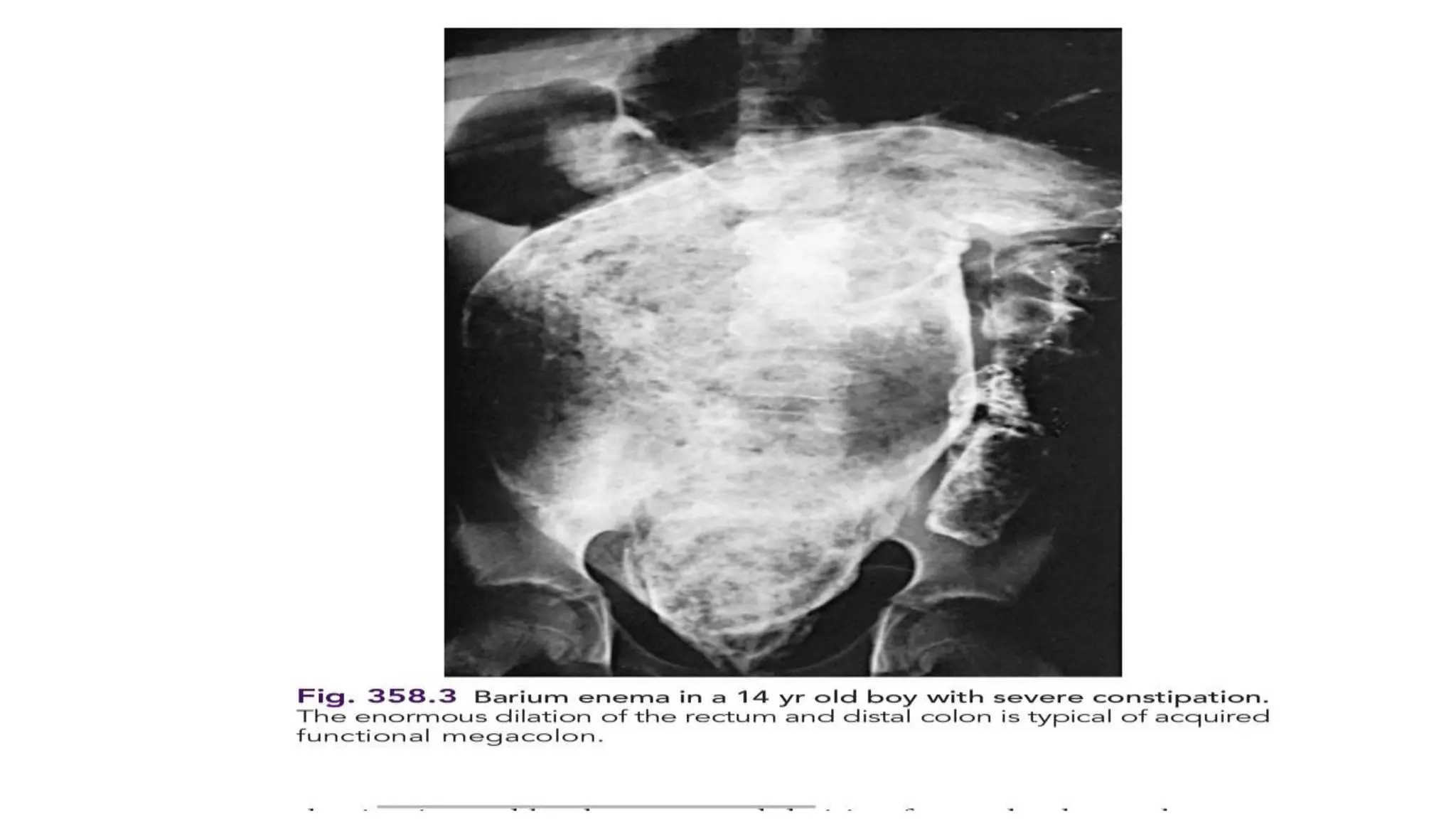
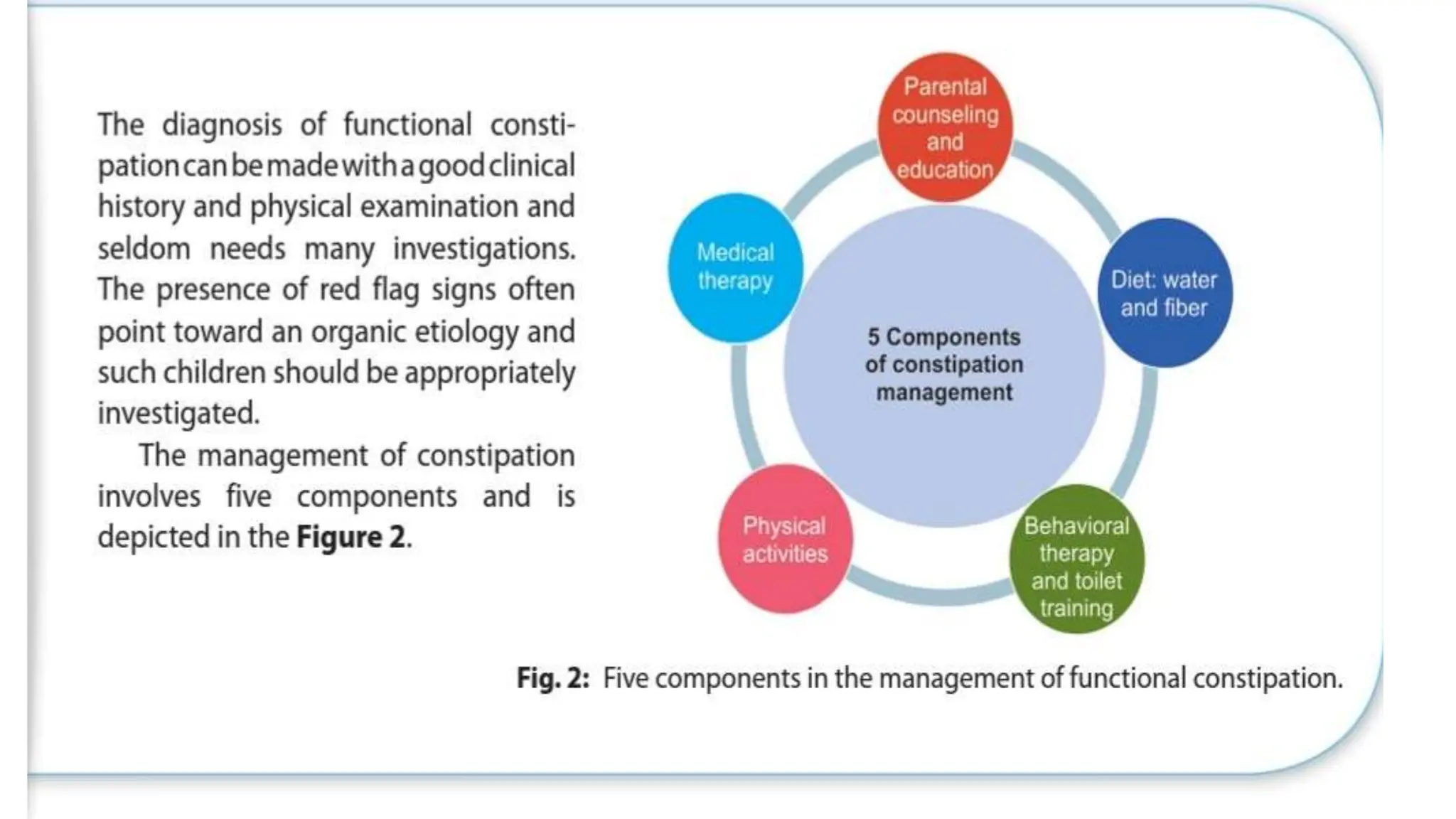
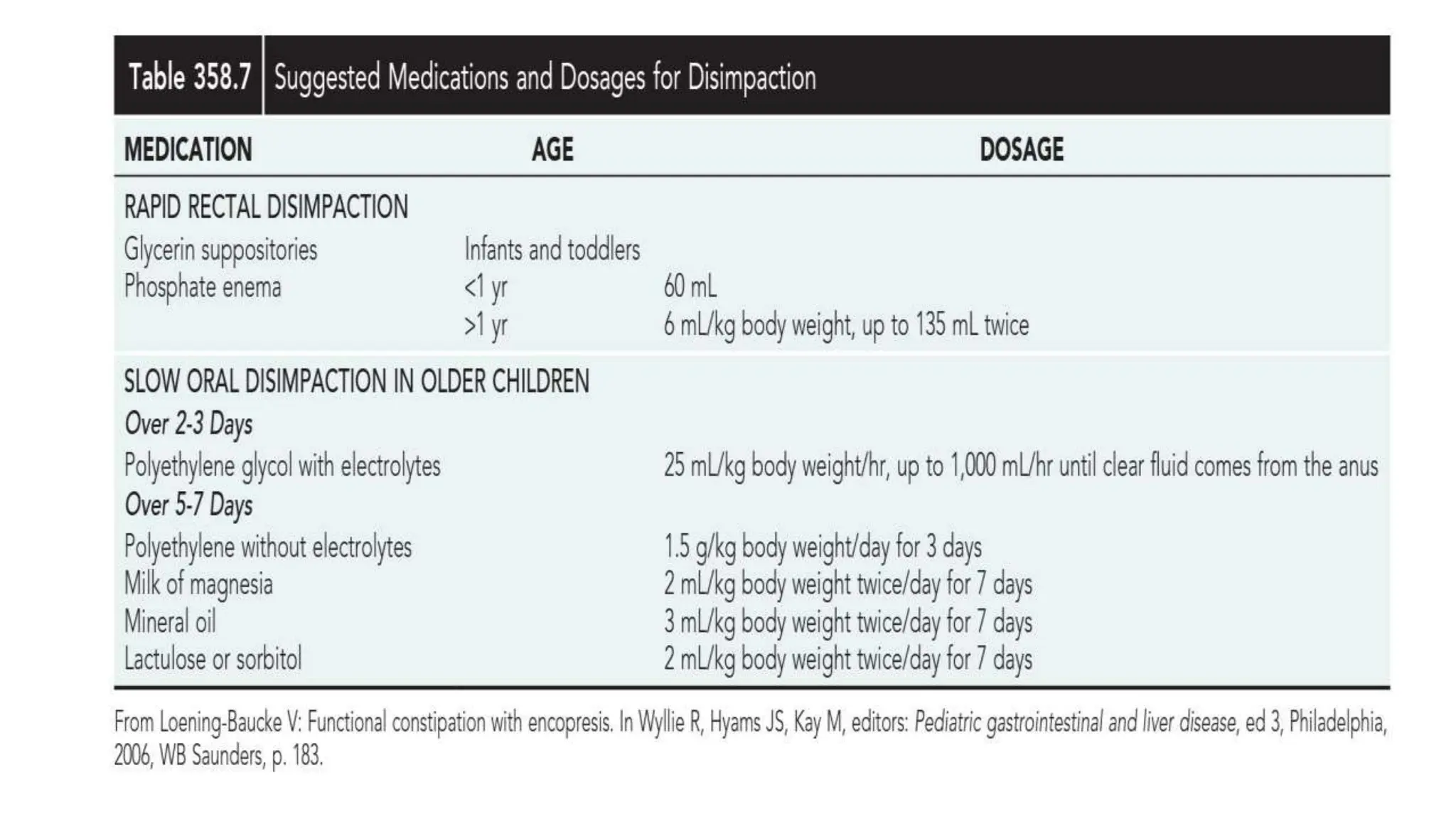
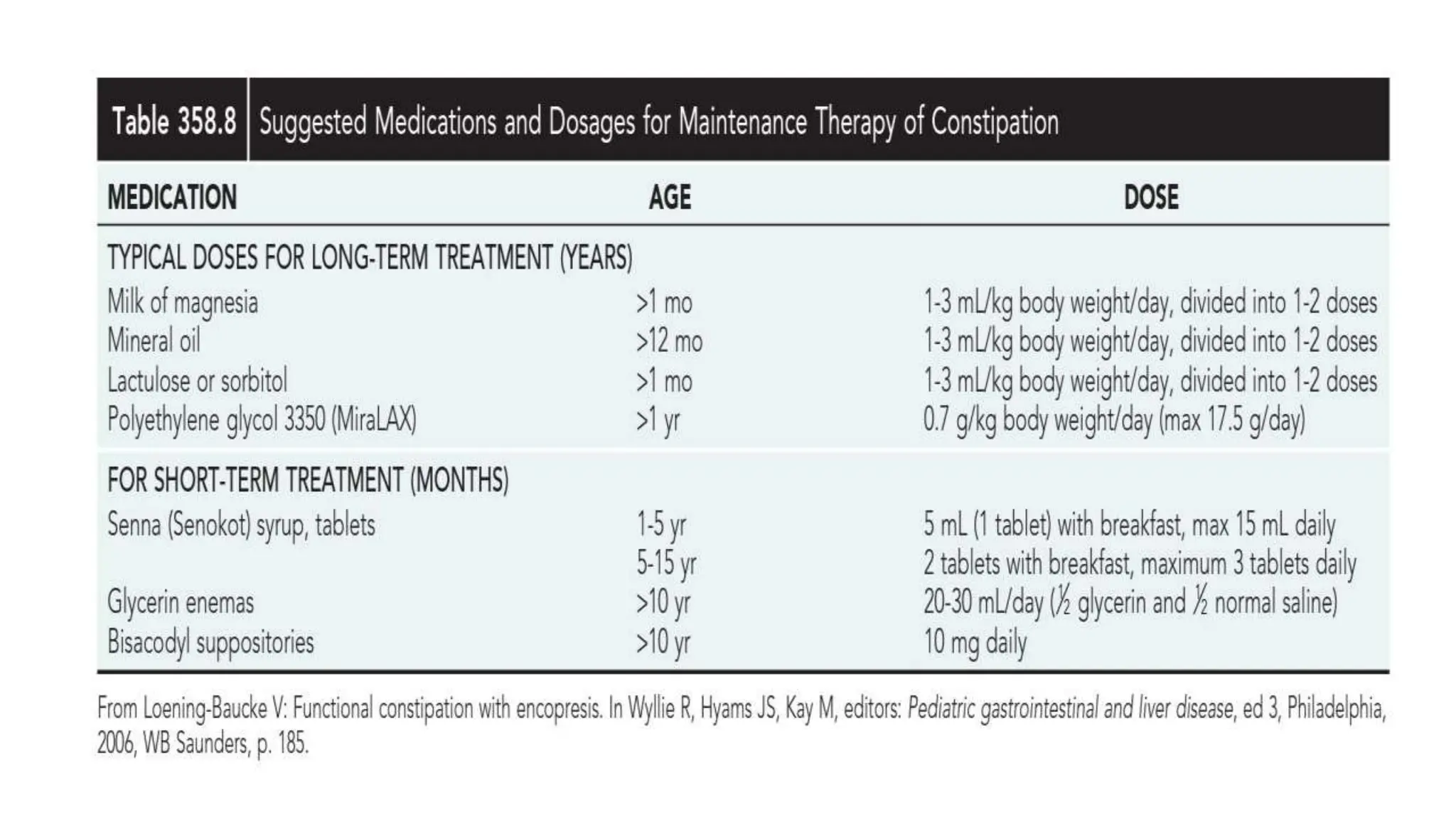
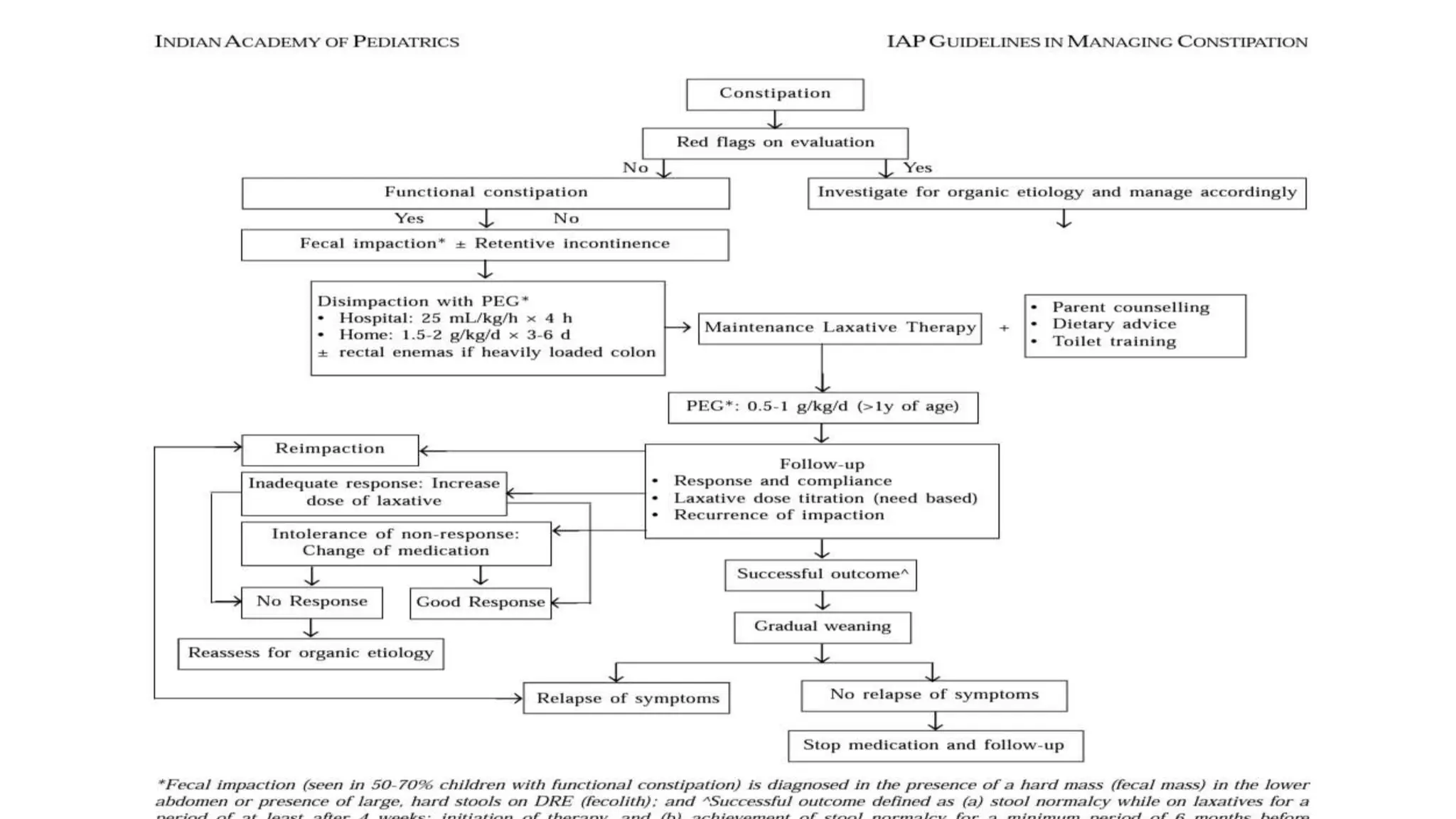
Functional constipation and encopresis can develop due to social stressors, dietary changes, inappropriate toilet training, or painful bowel movements establishing a cycle of retention. Management includes parental education, increasing fiber/water, exercise, proper toilet training, and medical therapy including disimpaction, stool softeners, and behavioral interventions. Chronic constipation may lead to a megarectum, and encopresis is the involuntary passage of feces occurring at least monthly for 3 months in children over age 4.