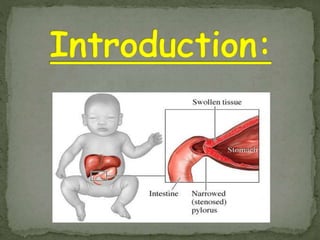
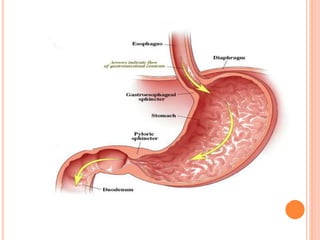
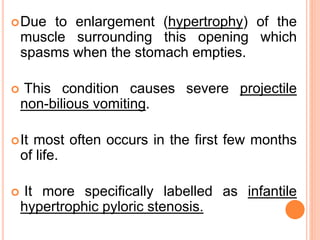
Pyloric stenosis is a narrowing of the opening from the stomach to the small intestine caused by thickening of the pyloric muscle. It typically presents in infants as projectile vomiting after feeding. Diagnosis is usually made clinically based on symptoms and feeling an olive-sized mass in the abdomen. Treatment involves initially stabilizing the infant followed by surgery to cut the thickened pyloric muscle. With timely diagnosis and treatment, prognosis is excellent with complete relief of symptoms and normal development. Nurses play an important role in pre and post-operative care including monitoring temperature, IV fluids, pain, and for any surgical complications.














































![PYLORIC_STENOSIS IN SICK CHILDREN[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pyloricstenosisinchildren1-240909081844-b3459eee-thumbnail.jpg?width=640&height=640&fit=bounds)









































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


