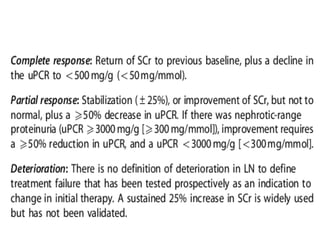
The document provides American College of Rheumatology guidelines for screening, treating, and managing lupus nephritis. It defines the disease burden, case definitions, and classifications. It recommends renal biopsy for untreated patients and outlines treatment principles based on disease classification. For classes III and IV, it recommends initial therapy with corticosteroids and immunosuppressants. It provides monitoring guidelines and addresses treatment of relapses, resistant disease, and different disease classes. The goal is to induce and maintain remission to prevent long-term kidney damage.