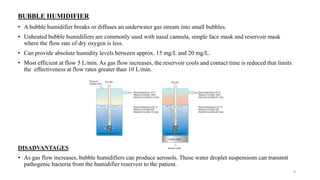
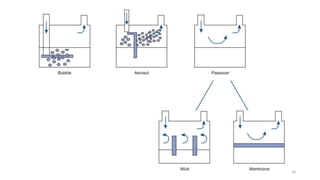
Humidification is important to condition inspired gases and maintain normal physiology in the lower airways. The nose normally warms and humidifies air, but other devices are needed when the upper airways are bypassed. Active humidifiers like bubble and passover humidifiers add heat and water, while passive heat-and-moisture exchangers conserve moisture from expiration. Proper humidification prevents complications like infection and inflammation by keeping the isothermic saturation boundary below the carina. Different devices are suitable for various situations depending on factors like gas flow and ability to provide adequate humidity without risk.