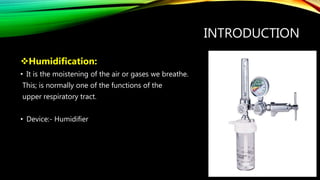
1. Humidification involves moistening the air or gases breathed in and is normally done by the upper respiratory tract, but mechanical humidifiers are needed when breathing through tubes or masks with added gases.
2. Different types of humidifiers include ambient temperature vapor suppliers, heated vapor suppliers, ambient aerosol suppliers, and heated aerosol suppliers. Heat and moisture exchangers also conserve water, heat, and moisture.
3. Humidification is important when breathing through endotracheal or tracheostomy tubes to prevent thick secretions, when breathing medical gases which are dry, and when secretions are abnormally thick to help their removal.
![HUMIDIFICATION
Dr. Rekha Marbate [PT]
Assistant Professor](https://image.slidesharecdn.com/humidification-211013092335/85/Humidification-1-320.jpg)












![• Sealed (to prevent contamination) water traps should be included in the circuit to
allow regular emptying without interrupting ventilation.
• A heated delivery tube eliminates the problem of condensation and allows the gas
to be delivered at a desired temperature of 32-36° with a water content of 33-43
g/m3 (Hinds & Watson 1996).
•
• Humiditiers can be used for the spontaneously breathing patient or can be
incorporated into ventilator circuits including continuous positive] airway pressure
and non-invasive ventilation](https://image.slidesharecdn.com/humidification-211013092335/85/Humidification-17-320.jpg)

































![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)




















![PT management in CKD [Renal Rehabilitation].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ptmanagementinckdrenalrehabilitation-220727071020-ee721238-thumbnail.jpg?width=640&height=640&fit=bounds)






































