Download as PPSX, PPTX







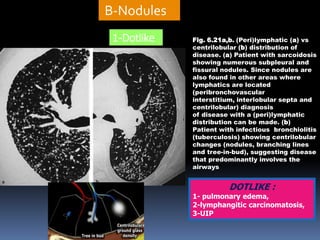


















1. The document provides guidance on interpreting chest CT scans by describing common patterns seen in interstitial lung diseases. 2. It outlines different types of nodules seen on CT scans including dot-like, ill-defined centrilobular, and tree-in-bud nodules and associates each with specific conditions. 3. The document also discusses the distribution of nodules and how this can provide clues to different diseases, such as perilymphatic nodules suggesting sarcoidosis.

































































































