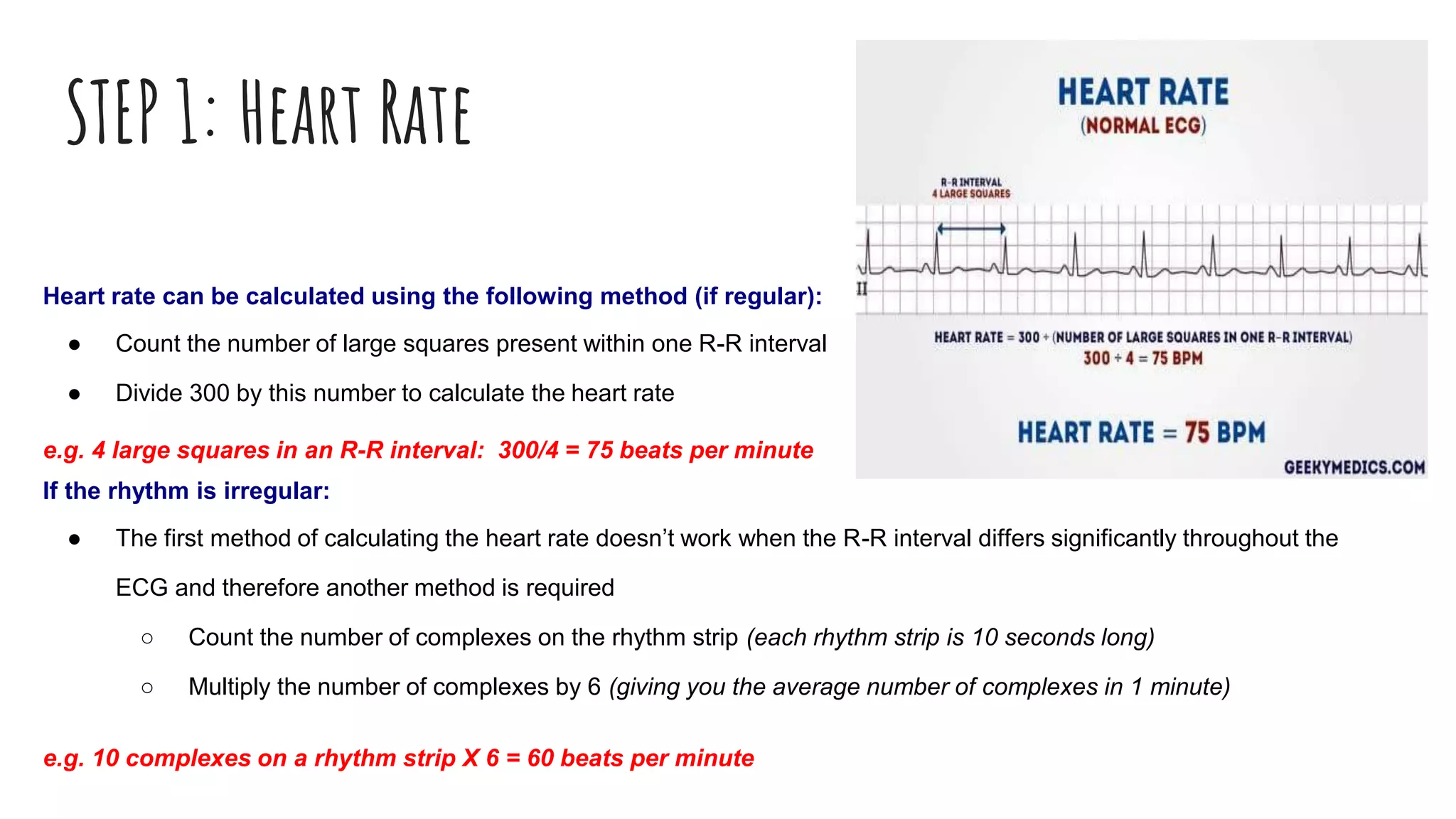
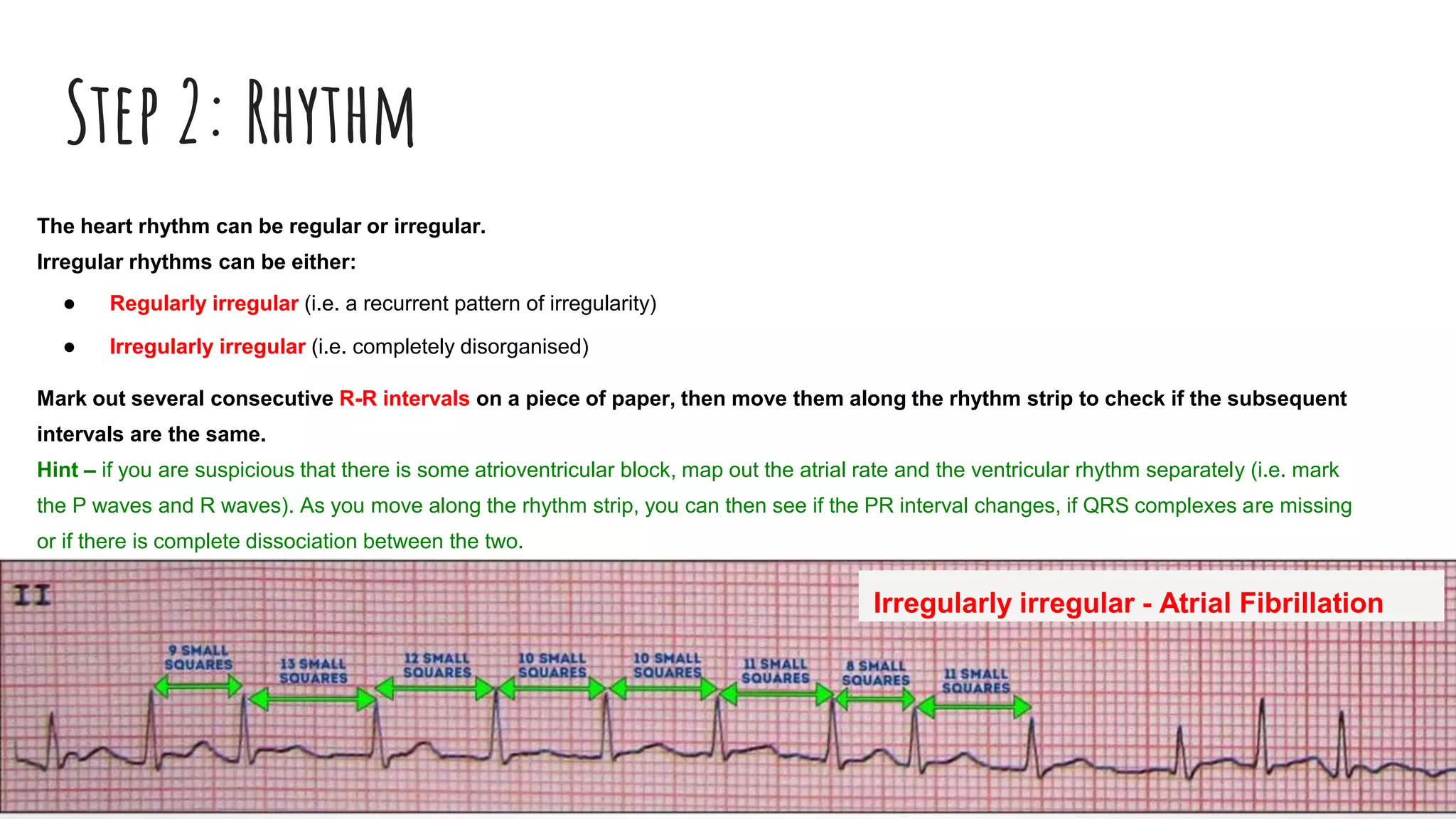
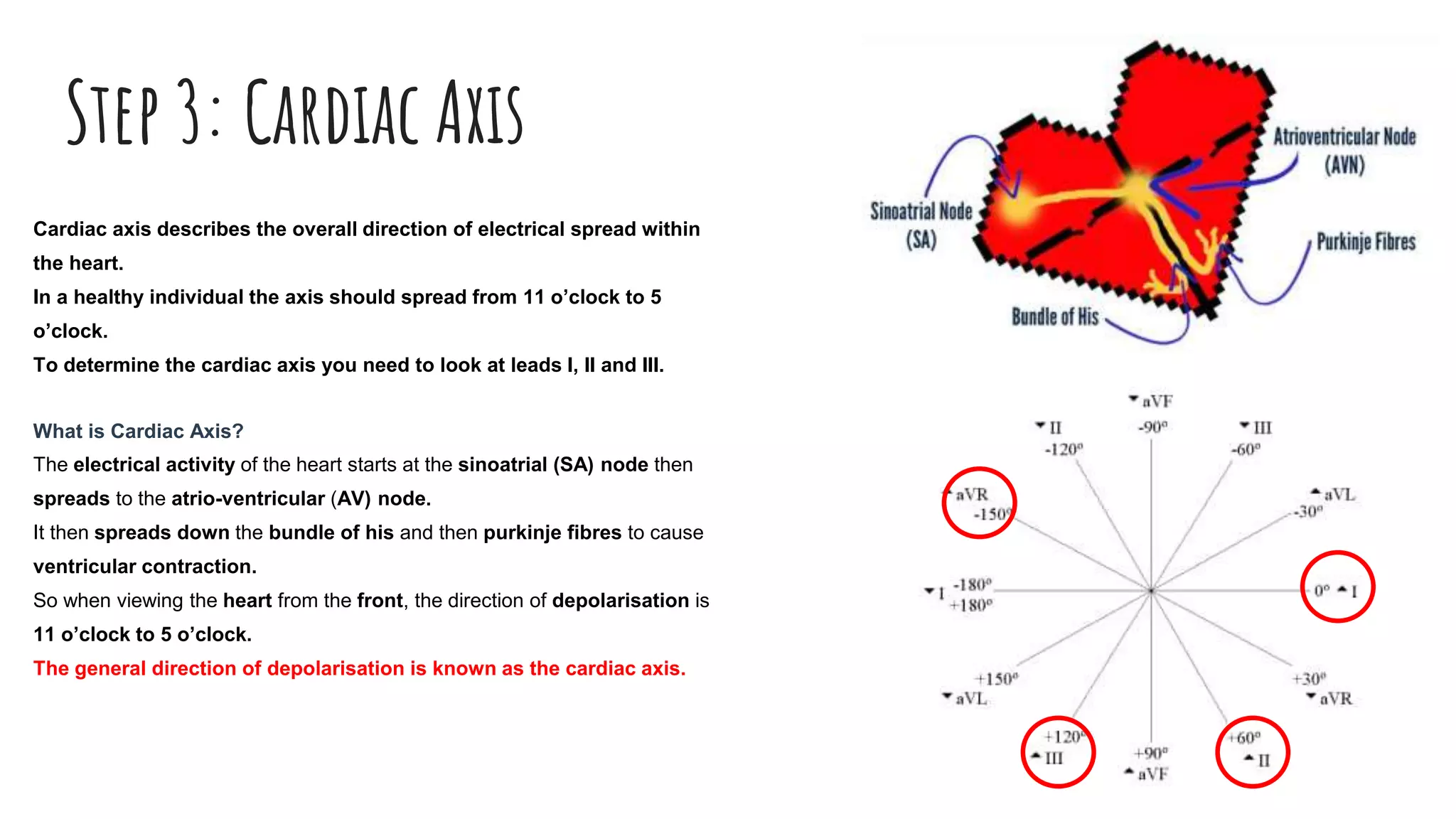
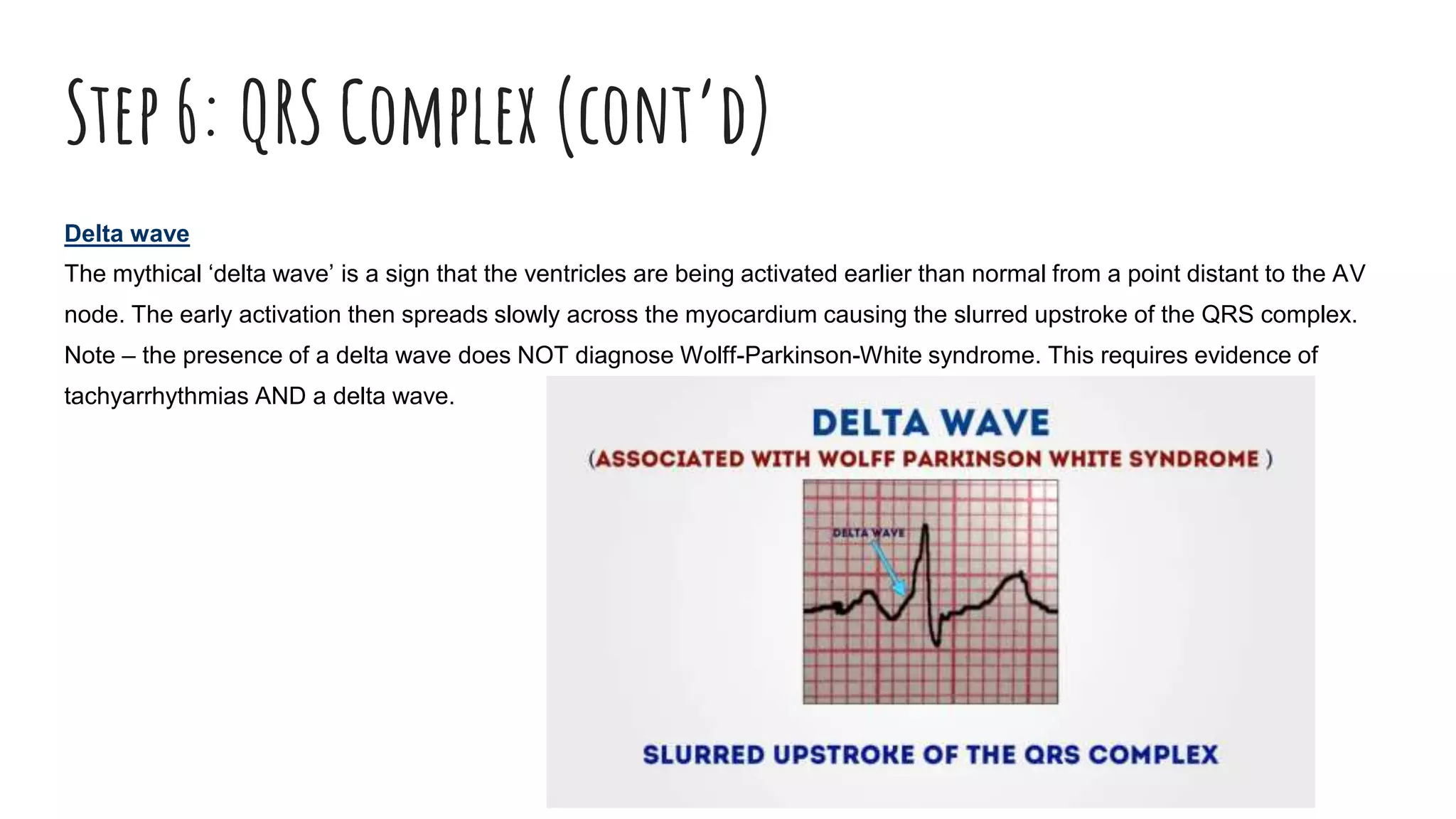
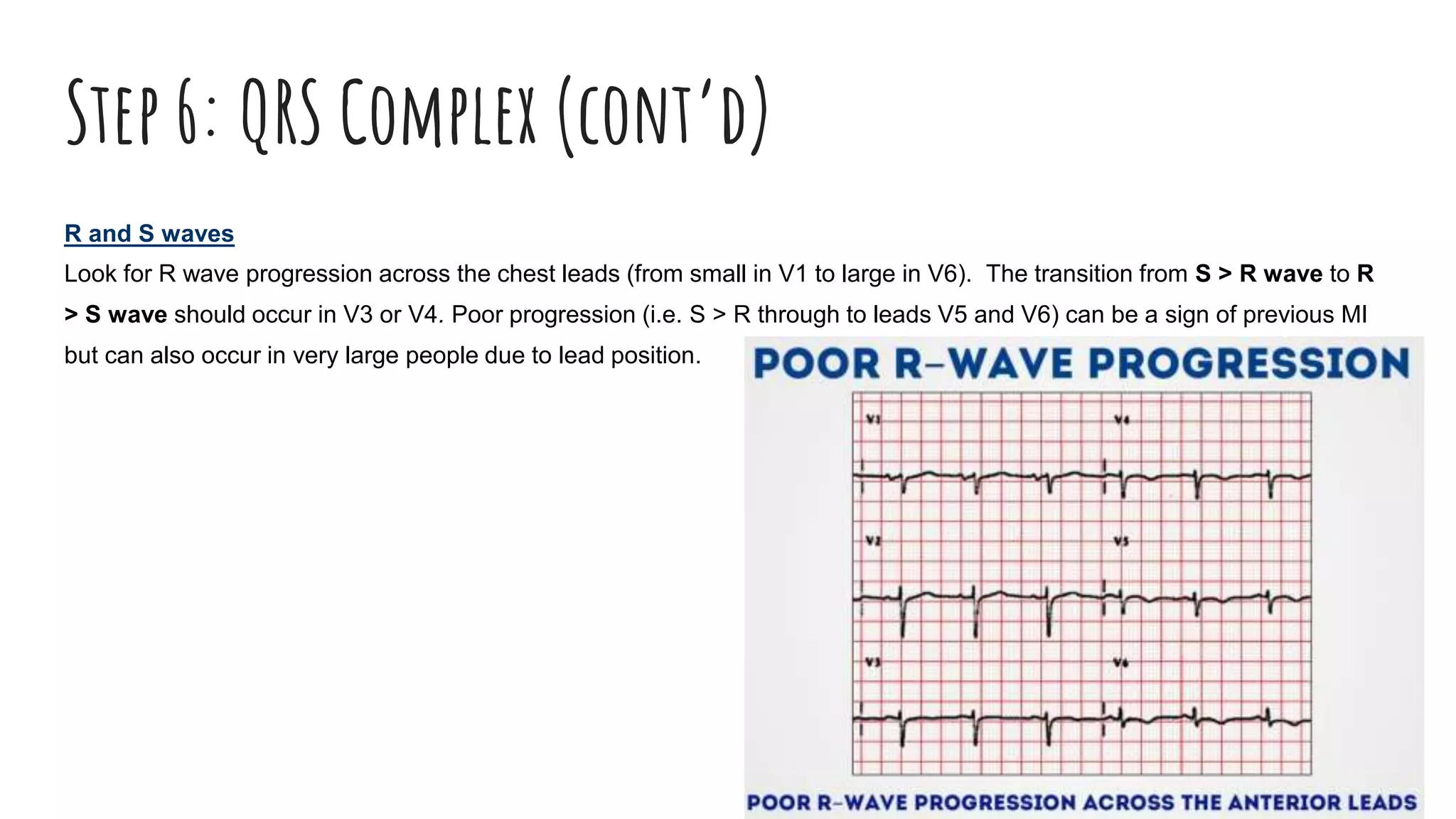
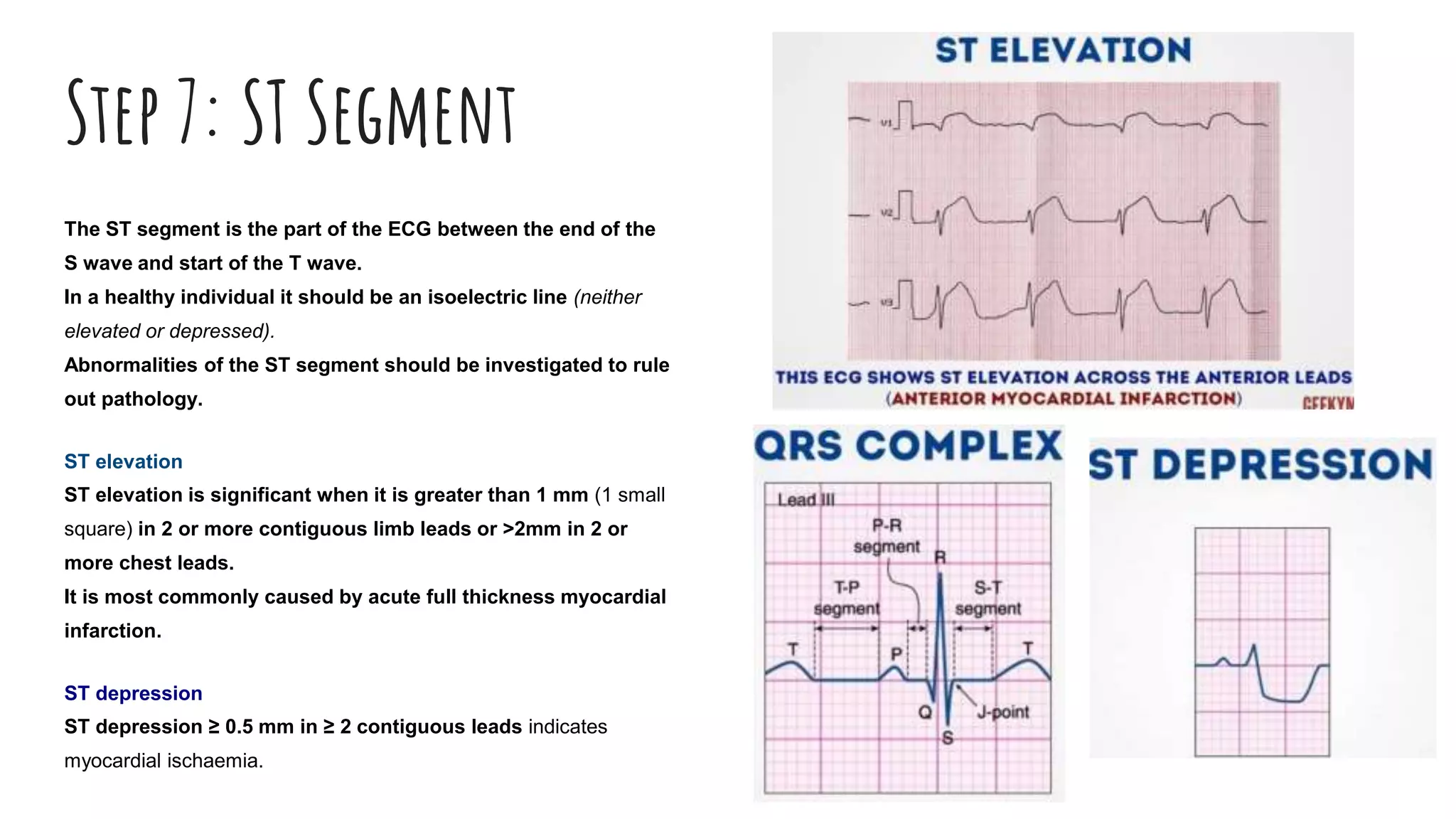
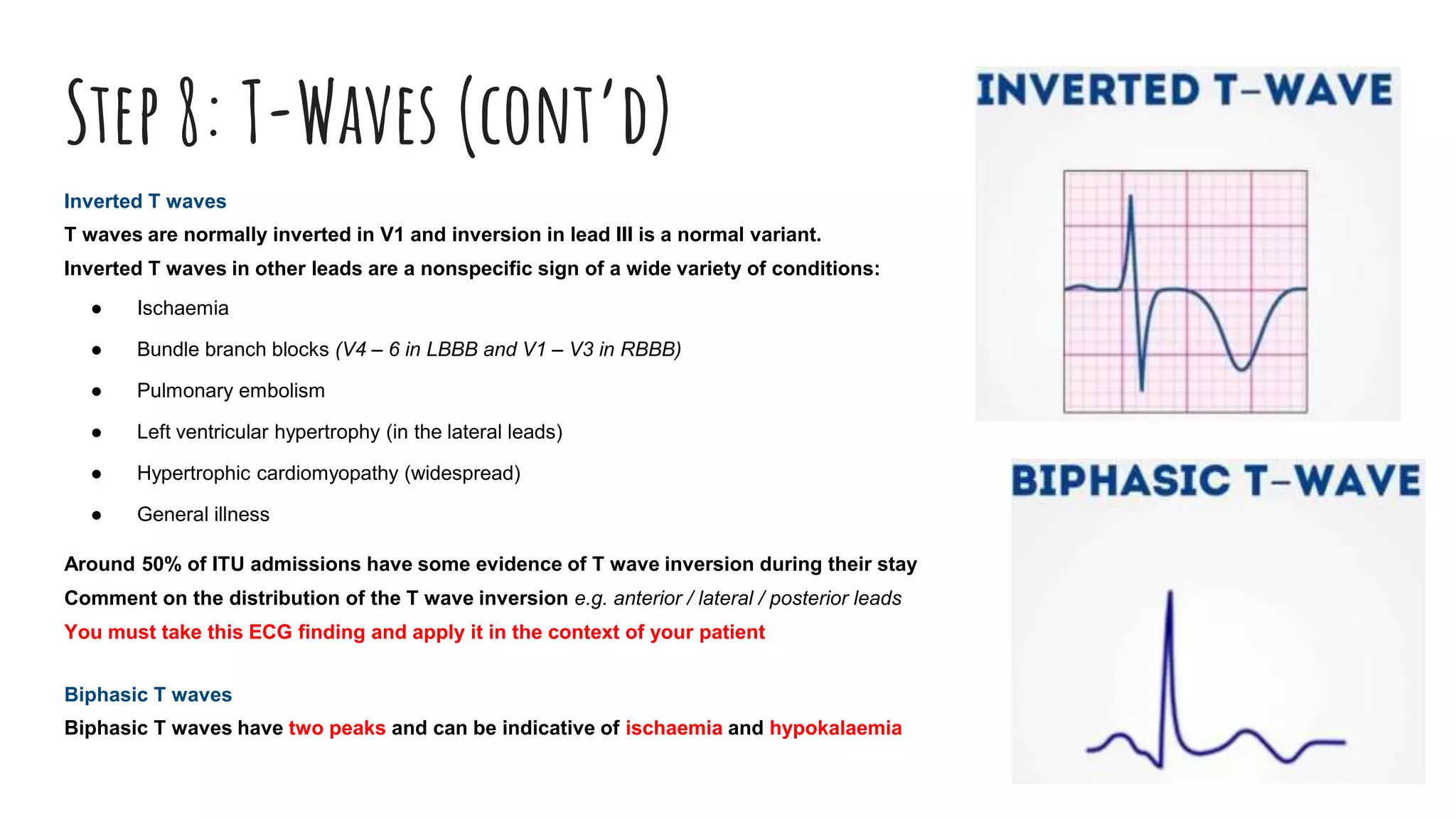
The document outlines a step-by-step process for reading an ECG, including calculating heart rate, assessing rhythm, cardiac axis, P waves, PR interval, QRS complex, ST segment, T waves, and U waves. Key items to evaluate at each step are identified, such as determining regular vs. irregular rhythm, signs of conduction abnormalities, and abnormalities that may indicate conditions like myocardial infarction. The overall goal is to systematically analyze all components of the E