Downloaded 13 times
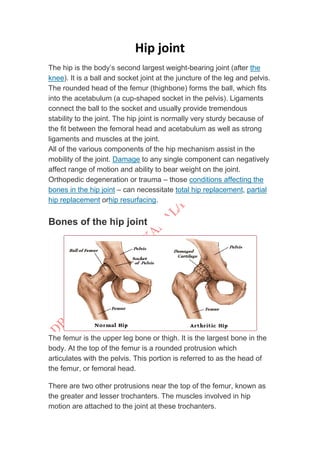















The hip joint is a ball and socket joint that connects the femur to the pelvis. It is the body's largest weight bearing joint. The rounded head of the femur fits into the cup-shaped acetabulum of the pelvis. Strong ligaments and muscles provide stability to the joint. Damage to any of the hip joint components can negatively affect its range of motion and weight bearing ability, and may require hip replacement surgery. The hip allows for flexion, extension, abduction, adduction, internal and external rotation.





































































































