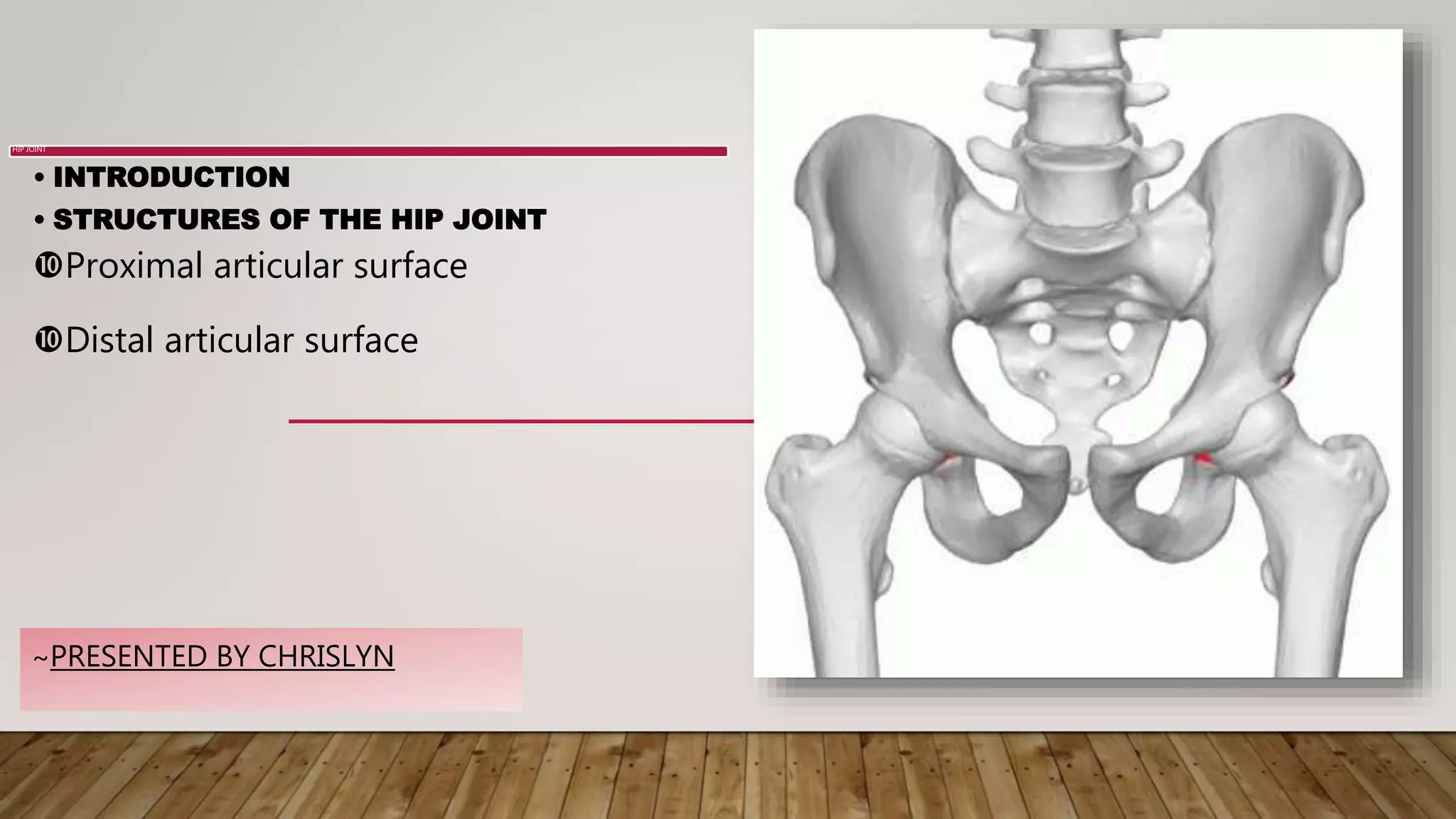
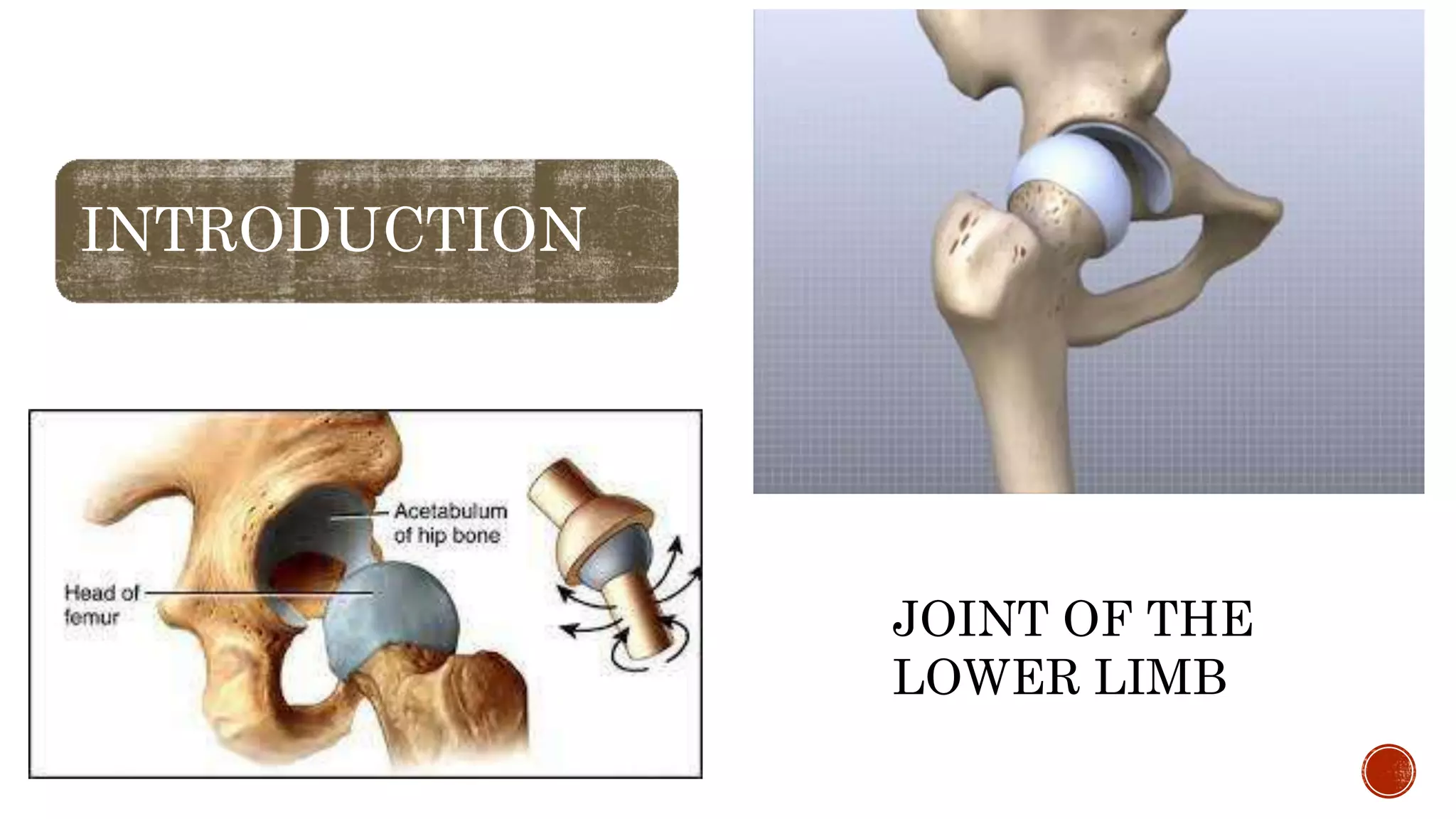
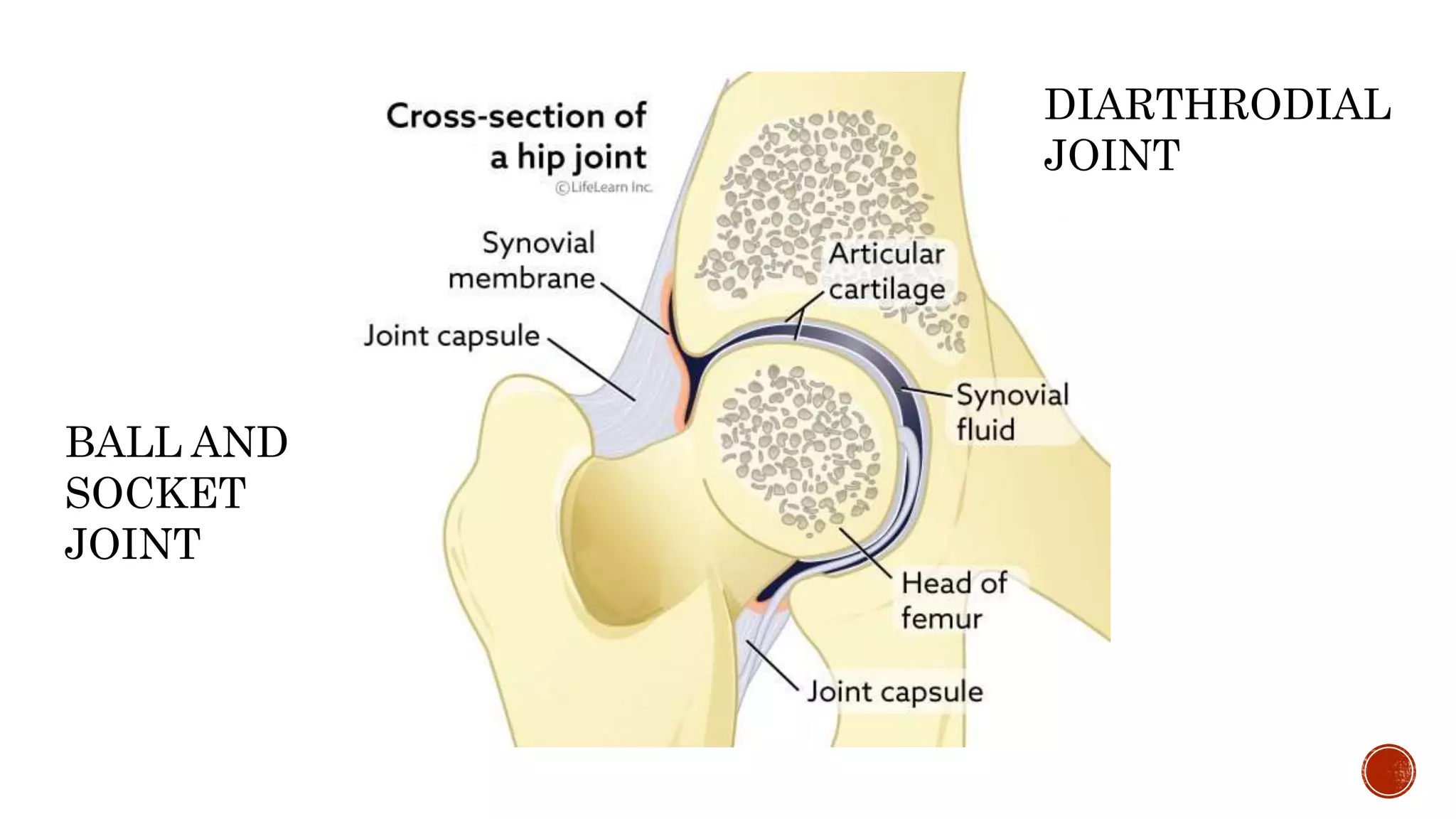
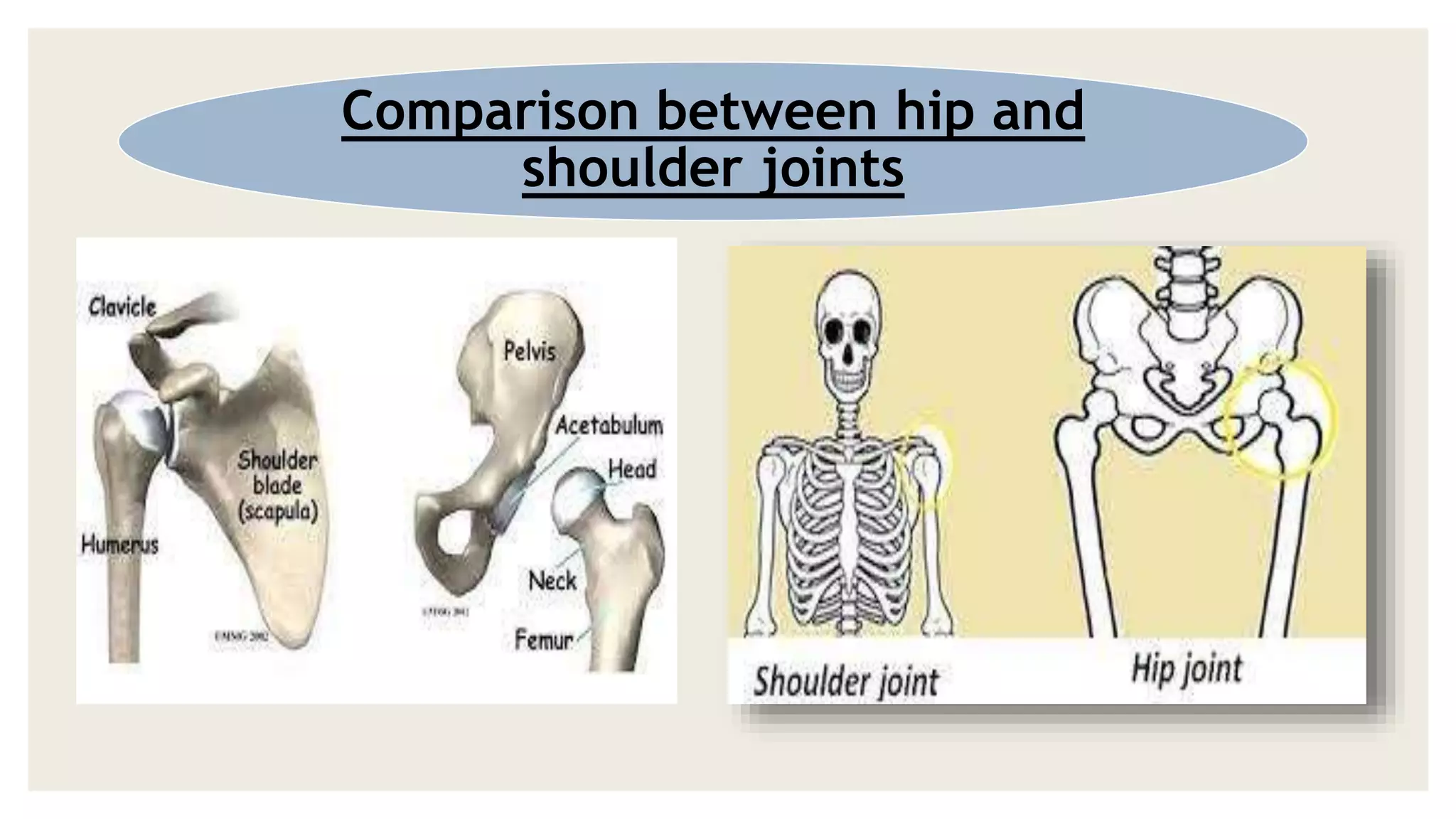
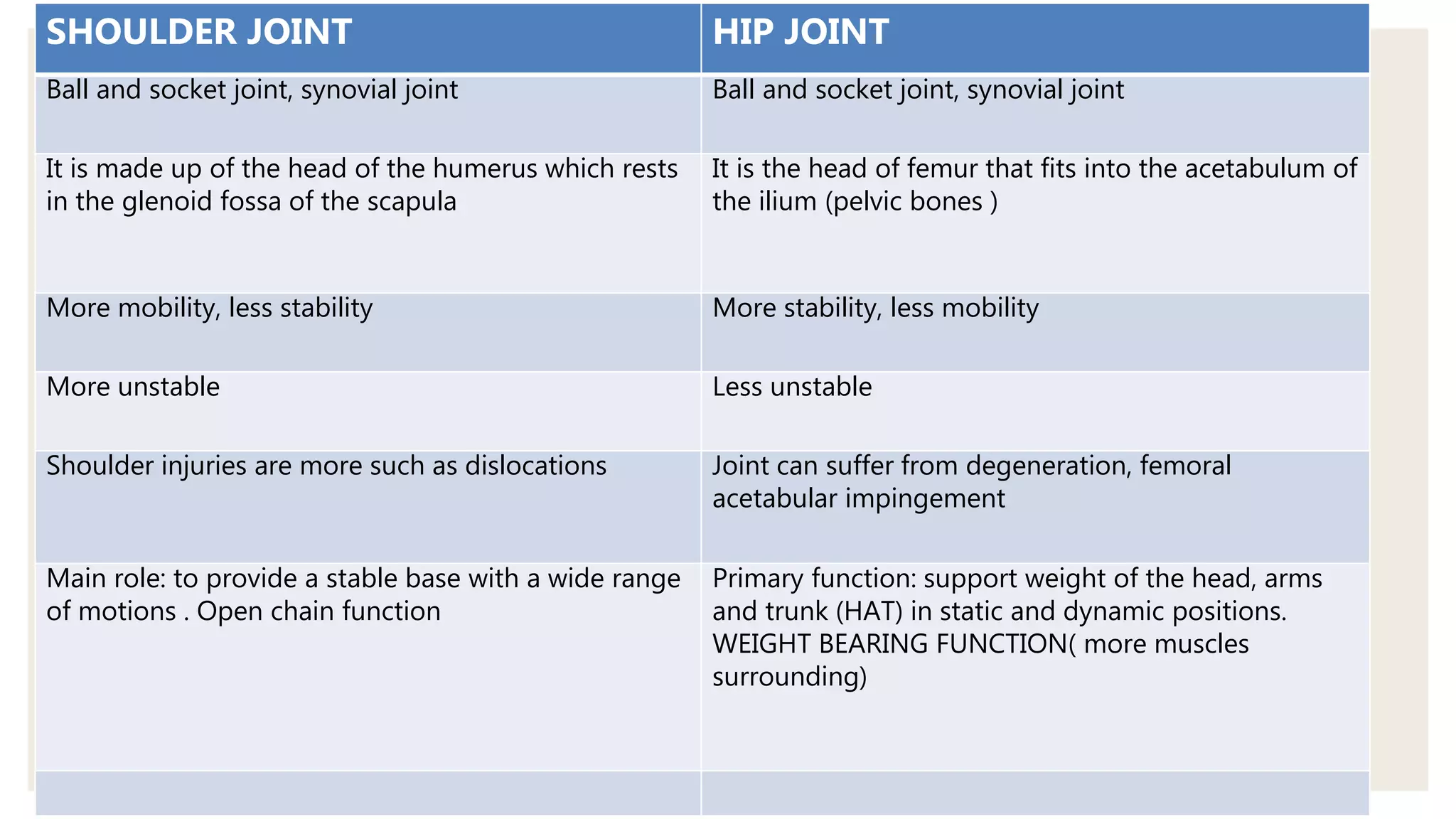
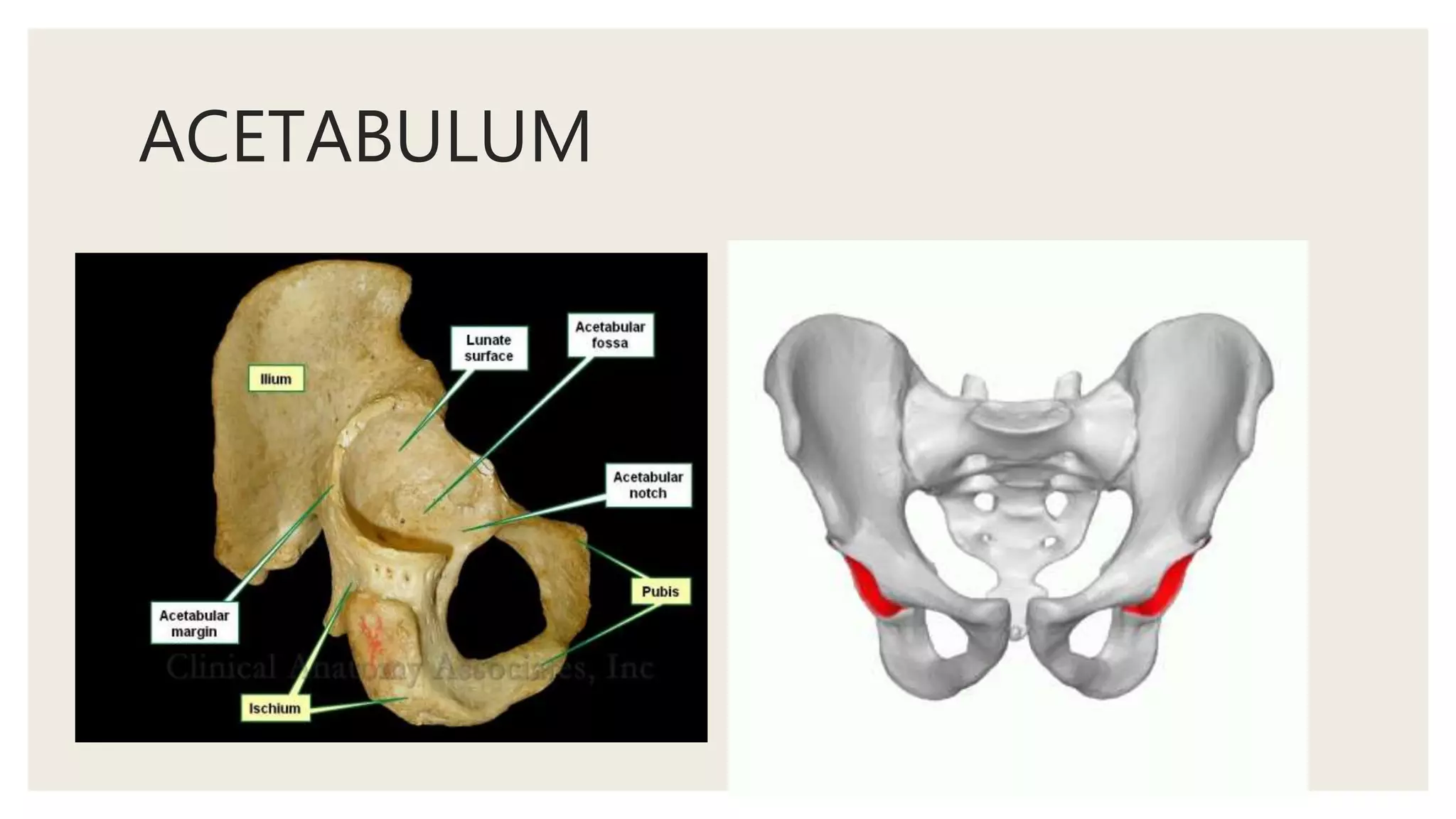
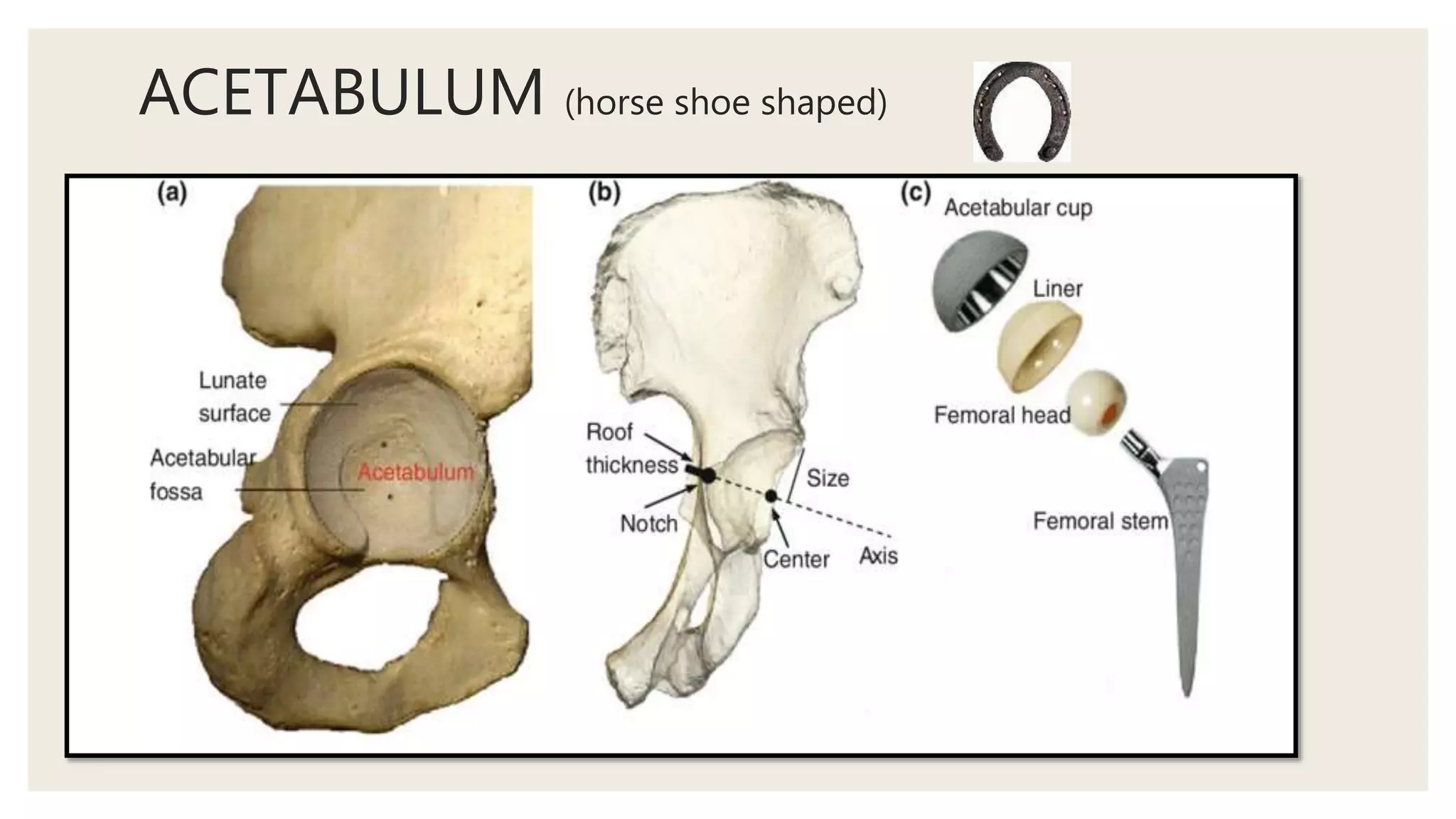
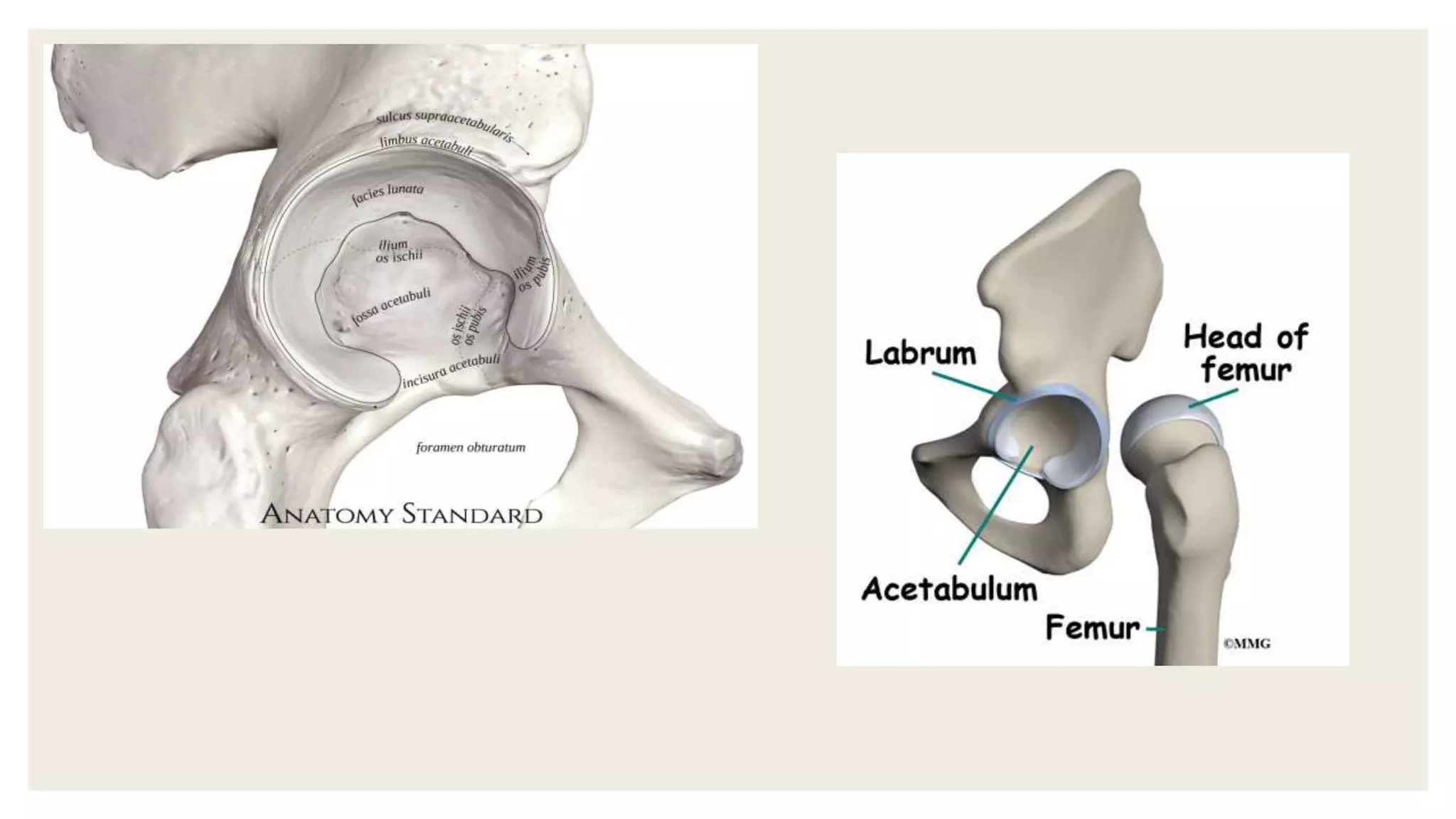
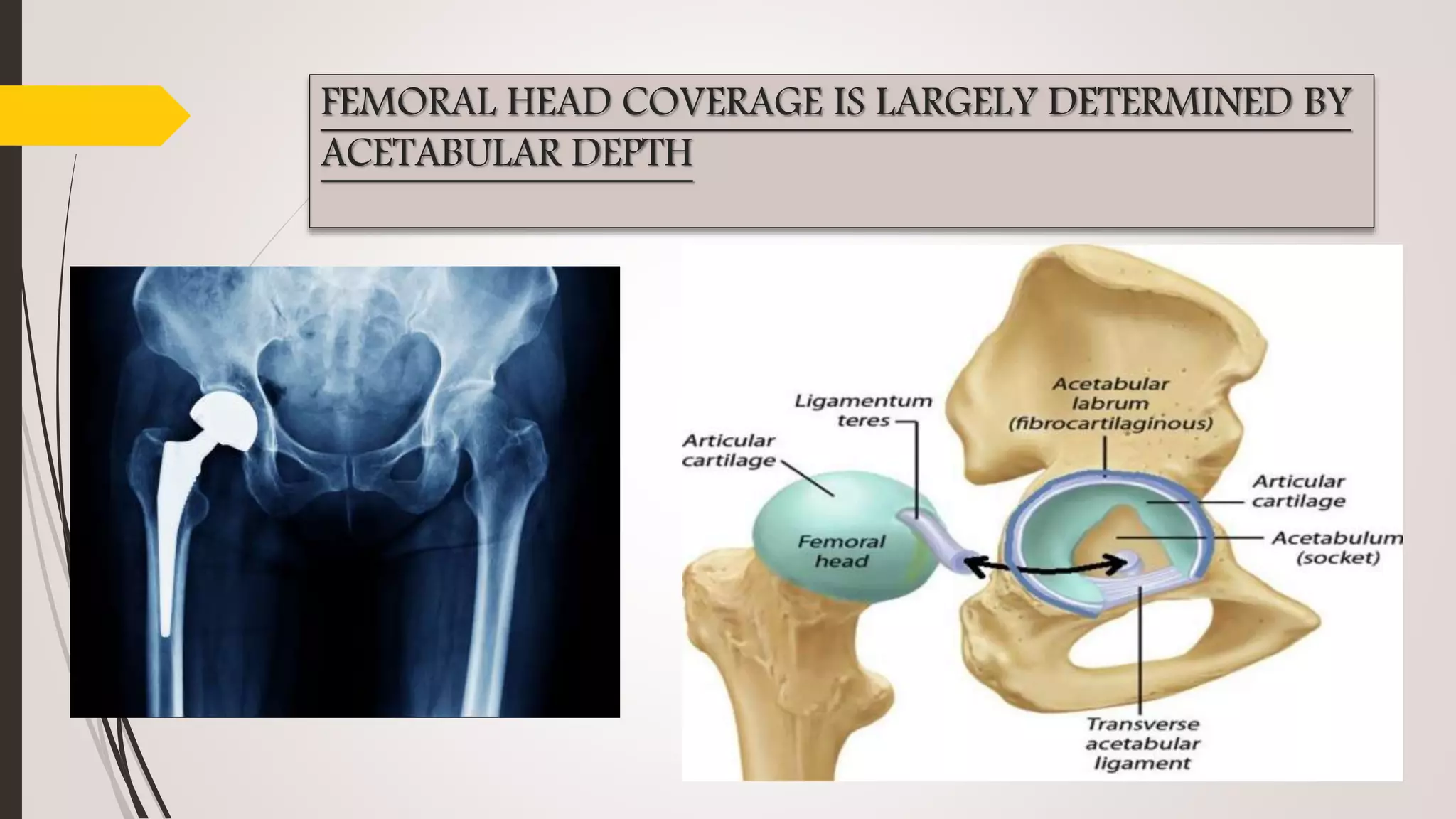
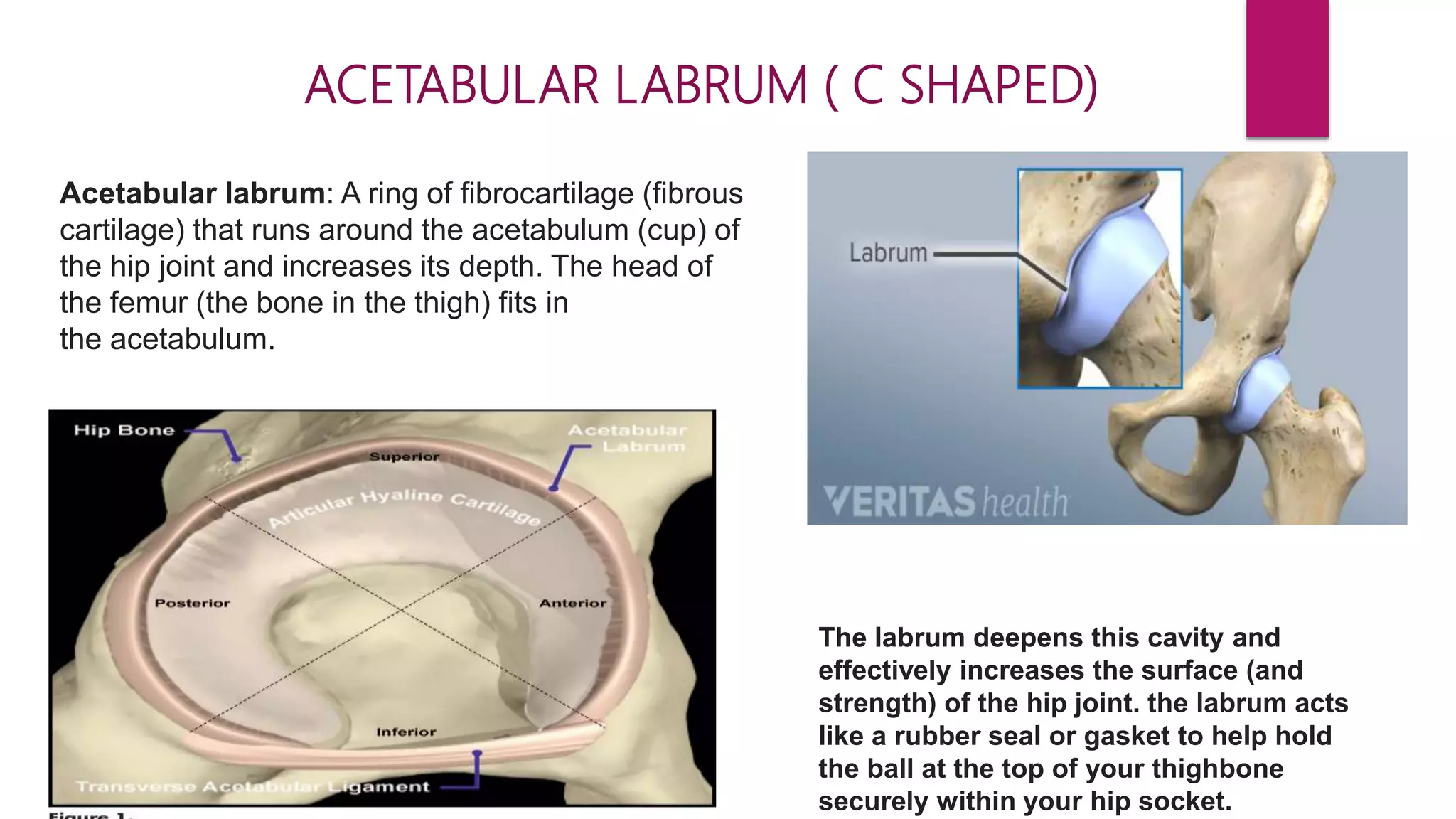
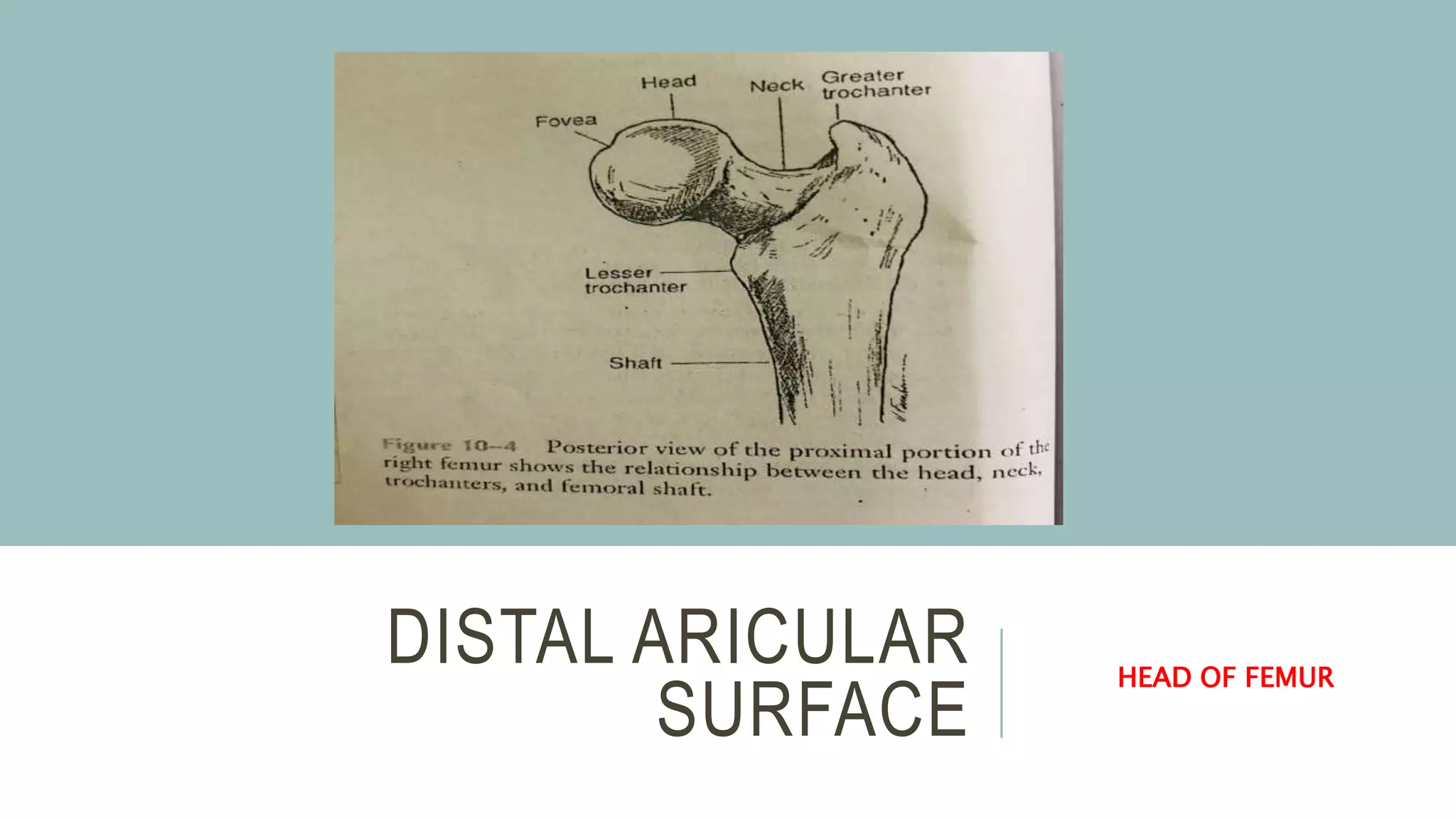
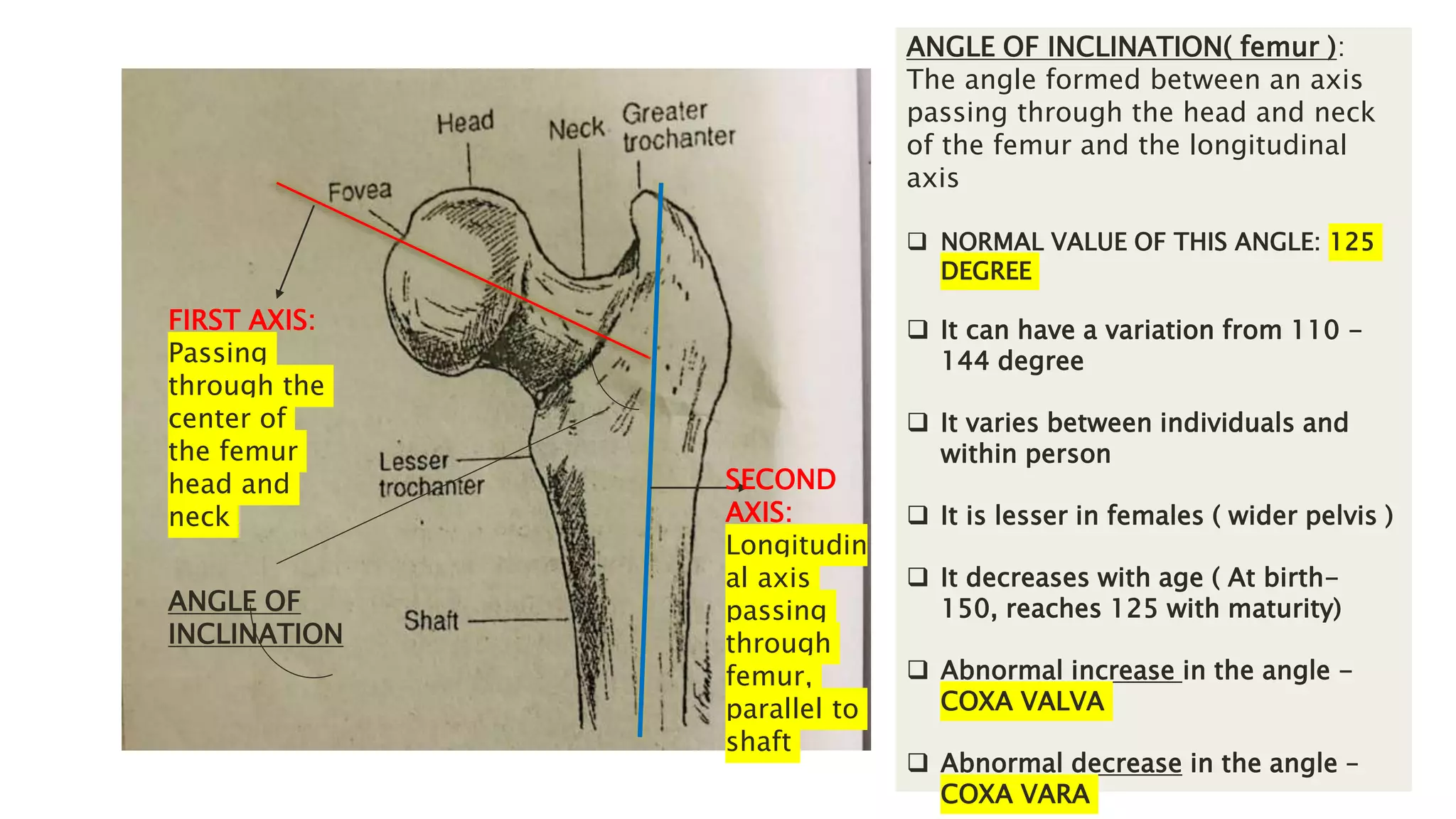
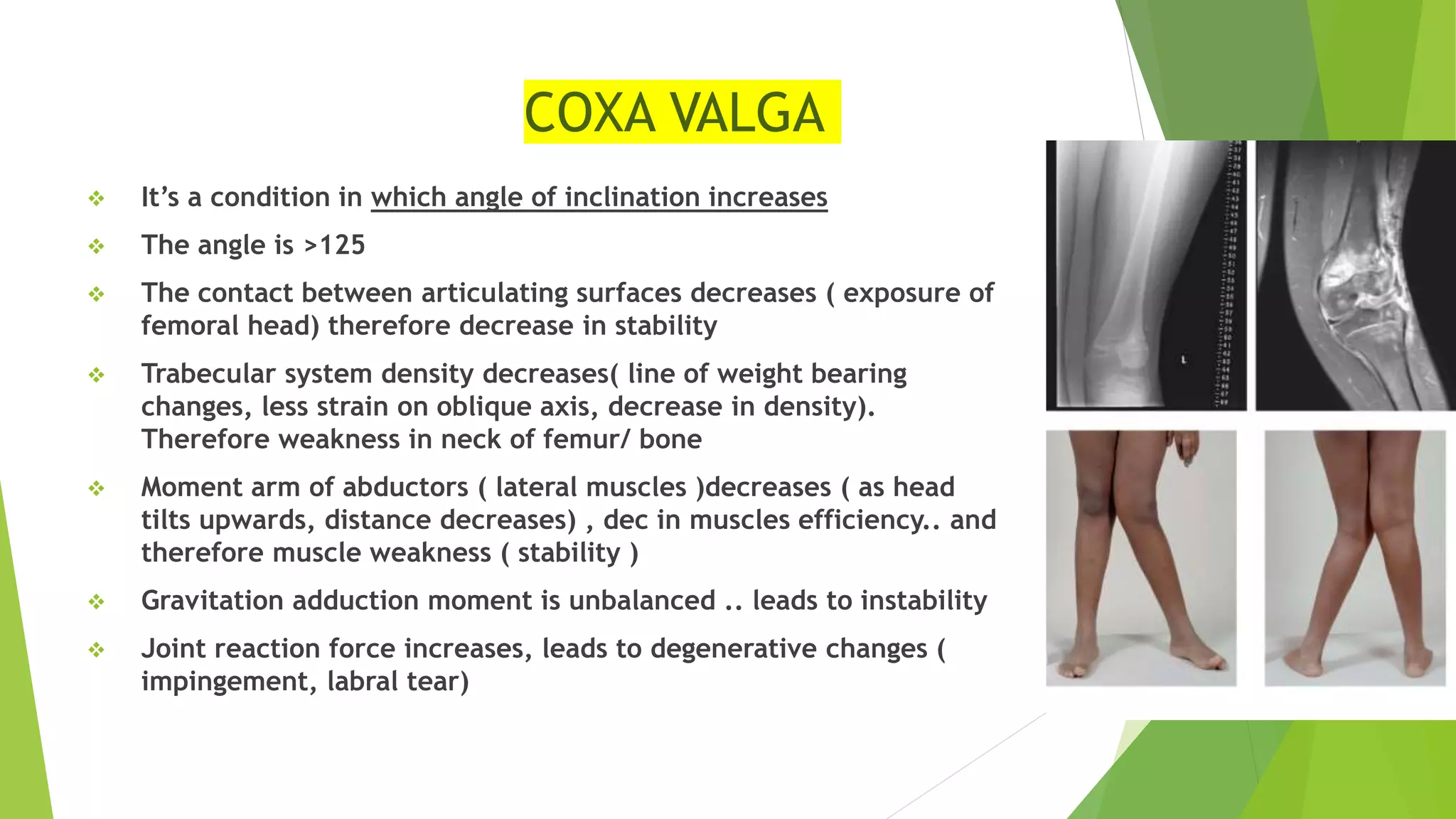
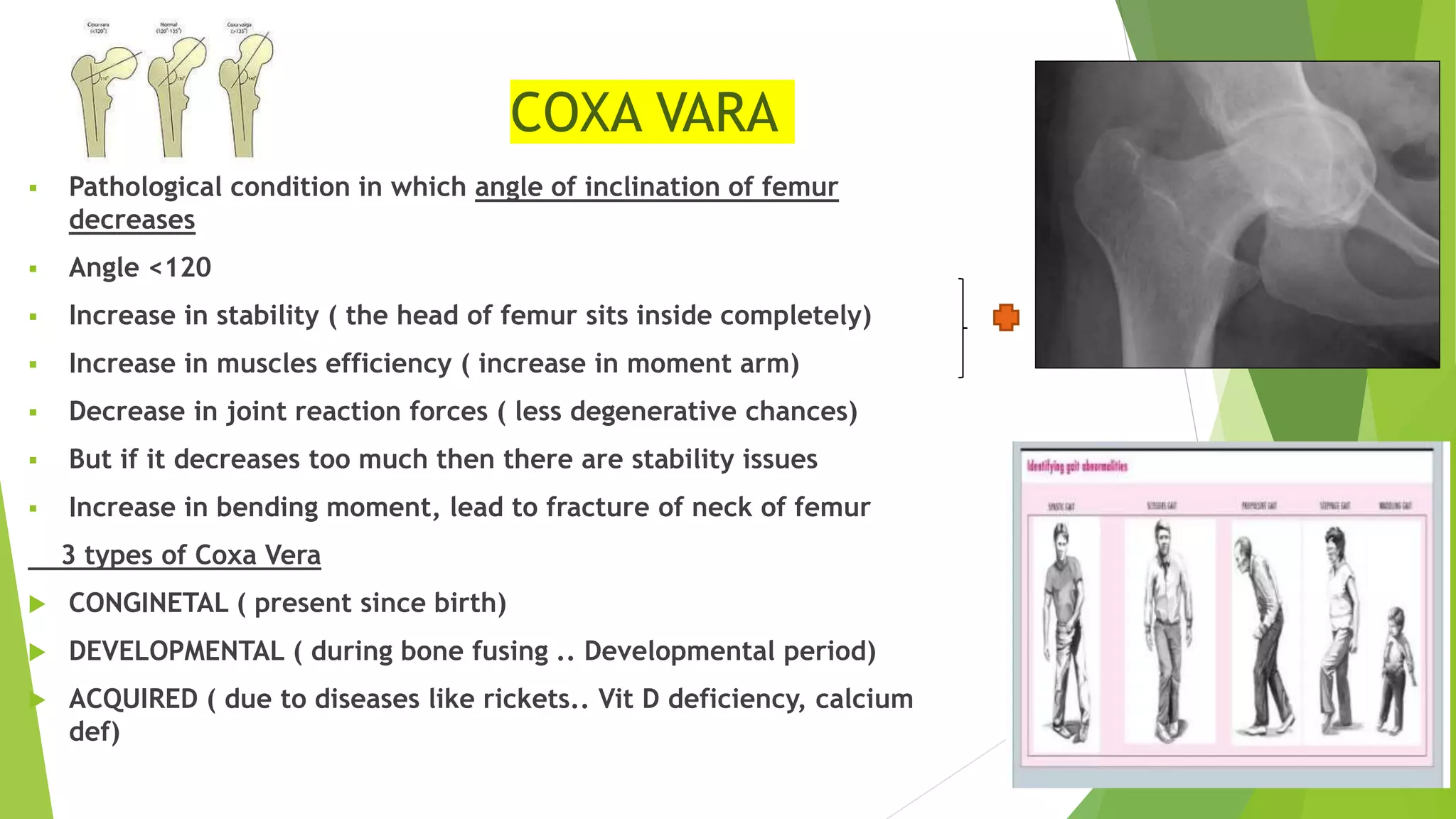
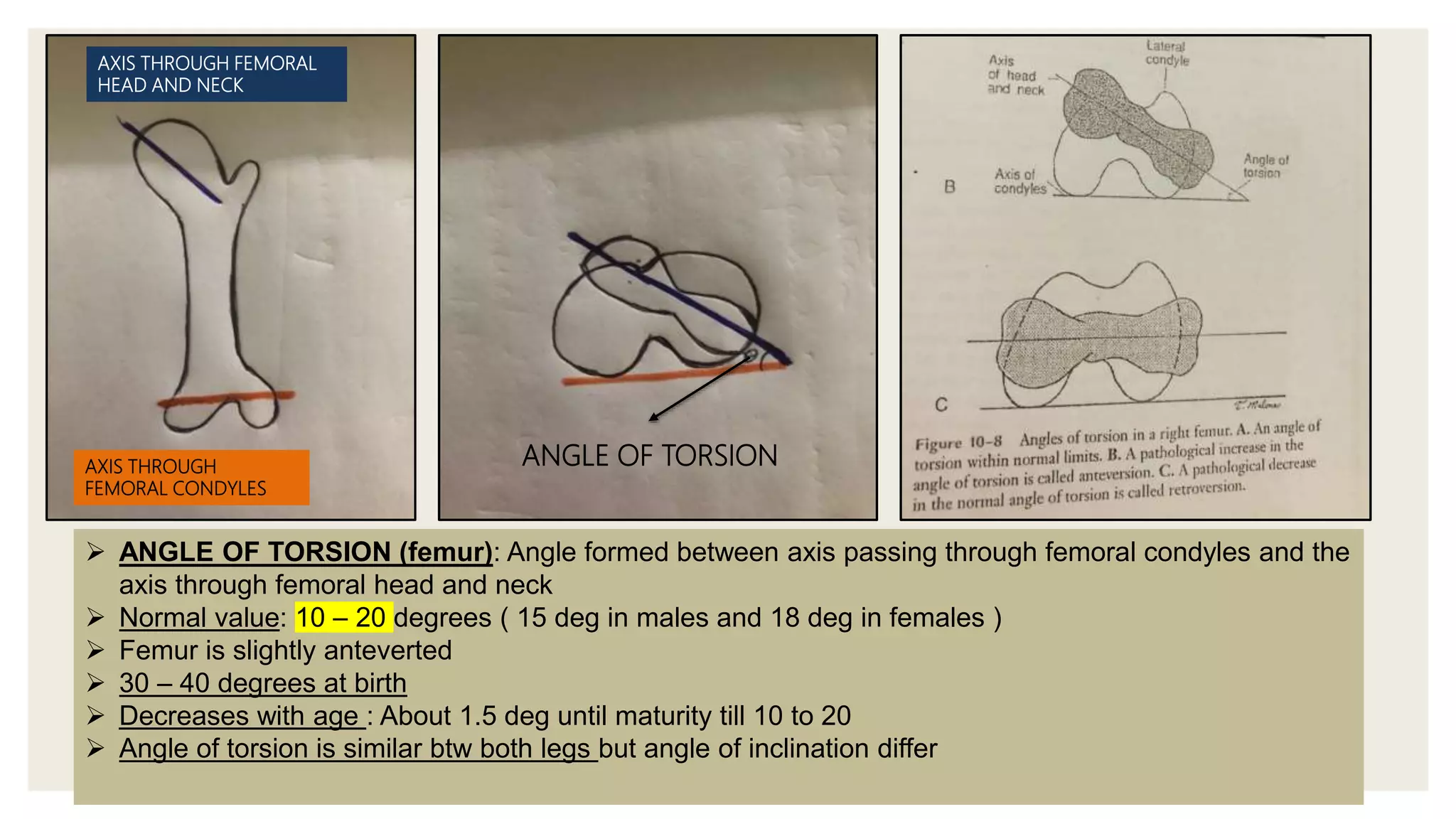
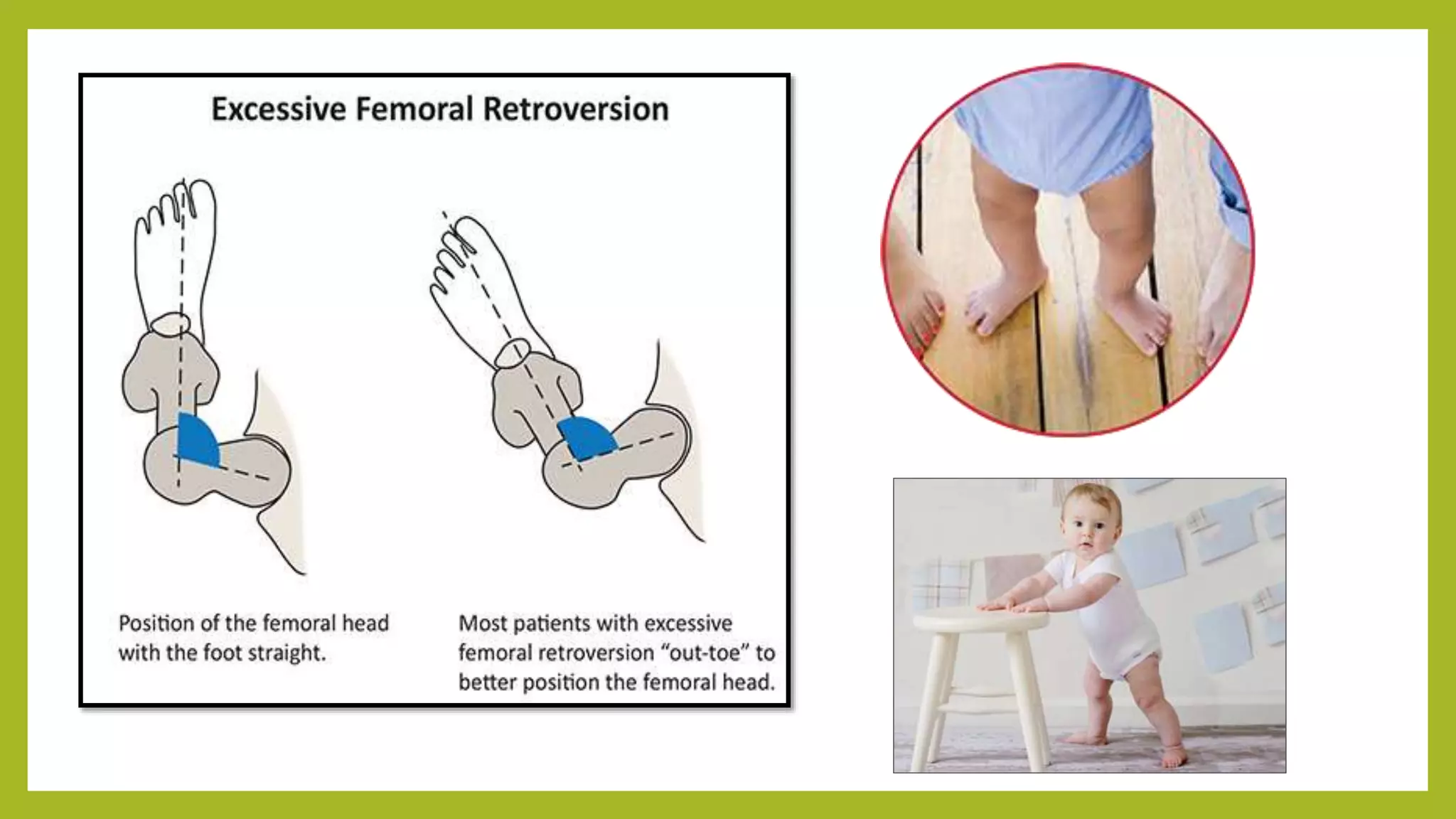
The hip joint is a ball and socket synovial joint that connects the femur to the pelvis. It has two articular surfaces: the proximal surface is the acetabulum of the pelvis, and the distal surface is the head of the femur. The acetabulum is cup-shaped and deepened by the acetabular labrum. The head of the femur fits into the acetabulum and is connected to the femoral shaft by the femoral neck. The angle of inclination and torsion of the femur can vary between individuals and abnormalities in these angles can impact joint mechanics and cause pathology.