Download as PDF, PPTX

















![FEMORAL ALIGNMENT
DYSFUNCTIONS
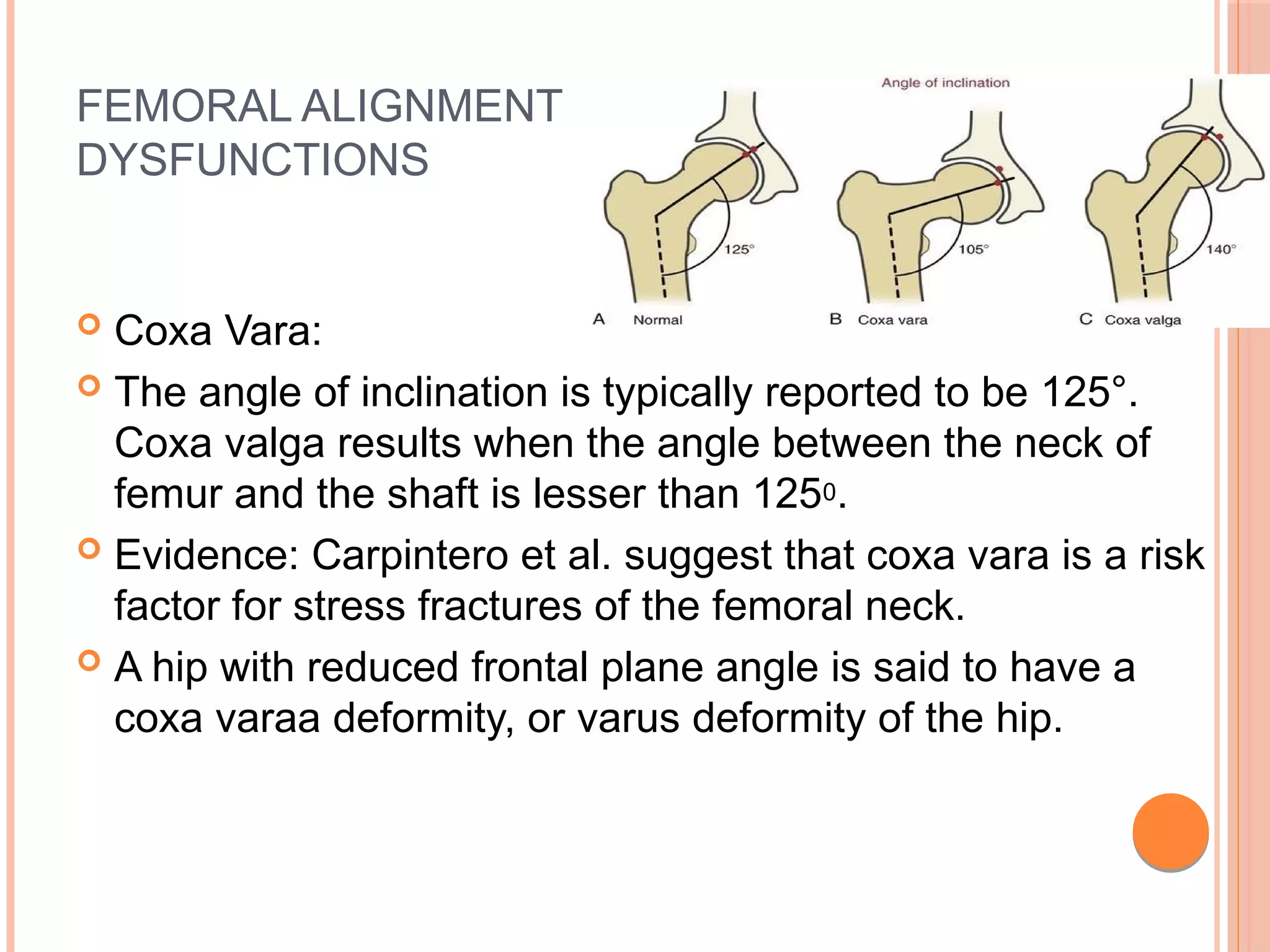
Coxa Valga:
As stated earlier, the angle of inclination is typically reported
to be 125°. Coxa valga results when the angle between the
neck of femur and the shaft is greater than 1250.
Evidence:
Yoshioka et al. report an average angle of 131°in a sample
of 32 cadaver specimens [72].
A hip with an excessive frontal plane angle is said to have a
coxa valga deformity, or valgus deformity of the hip.
HIP PATHOLOGY AND PATHOMECHANICSHIP PATHOLOGY AND PATHOMECHANICS](https://image.slidesharecdn.com/hipjointbioandpathomechanics-200414101544/75/Hip-joint-biomechanics-and-pathomechanics-46-2048.jpg)


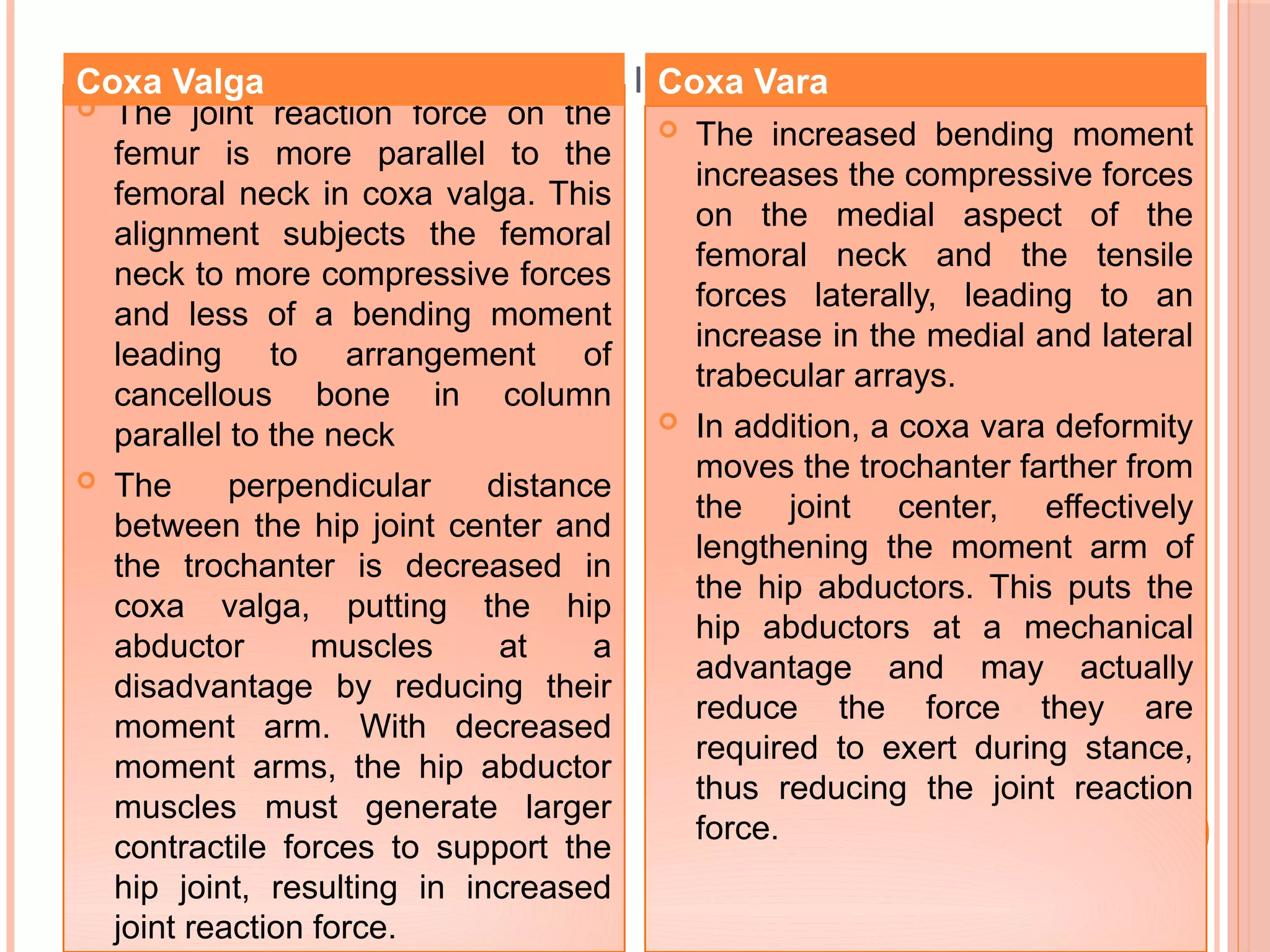
![BIOMECHANICAL ADVANTAGES IN THE HIP JOINT DEFORMITIES
In addition, the joint reaction
force is displaced laterally in
the acetabulum and is applied
over a smaller joint surface,
leading to increased joint
stress. In other words, coxa
valga deformities are likely to
increase the risk of
degenerative joint disease
within the hip by increasing the
joint reaction force as well as
the stress sustained by the
femoral head.
In addition, the joint reaction
force is displaced laterally in
the acetabulum and is applied
over a smaller joint surface,
leading to increased joint
stress. In other words, coxa
valga deformities are likely to
increase the risk of
degenerative joint disease
within the hip by increasing the
joint reaction force as well as
the stress sustained by the
femoral head.
However, coxa vara tends to
increase the medial pull on the
femur into the acetabulum, which
may contribute to erosion of the
acetabulum. Additionally, an
increased advantage for the
abductor muscles may be
accompanied by fatigue in the
antagonist muscles [5]. The
moment arm of the joint reaction
force may also be increased with
a net result of an increased
bending moment on the femoral
neck
However, coxa vara tends to
increase the medial pull on the
femur into the acetabulum, which
may contribute to erosion of the
acetabulum. Additionally, an
increased advantage for the
abductor muscles may be
accompanied by fatigue in the
antagonist muscles [5]. The
moment arm of the joint reaction
force may also be increased with
a net result of an increased
bending moment on the femoral
neck
Coxa Valga Coxa Vara](https://image.slidesharecdn.com/hipjointbioandpathomechanics-200414101544/75/Hip-joint-biomechanics-and-pathomechanics-51-2048.jpg)








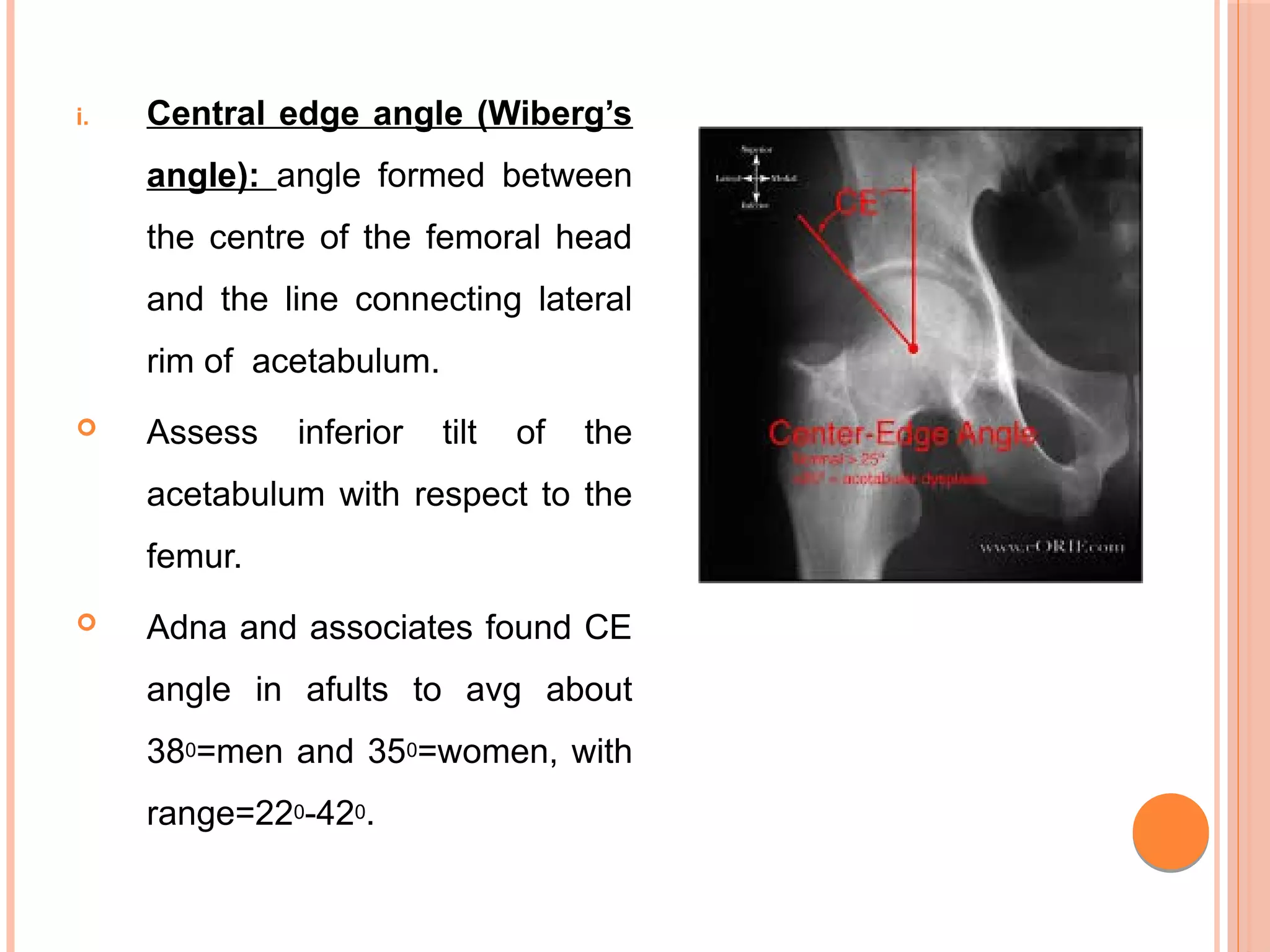
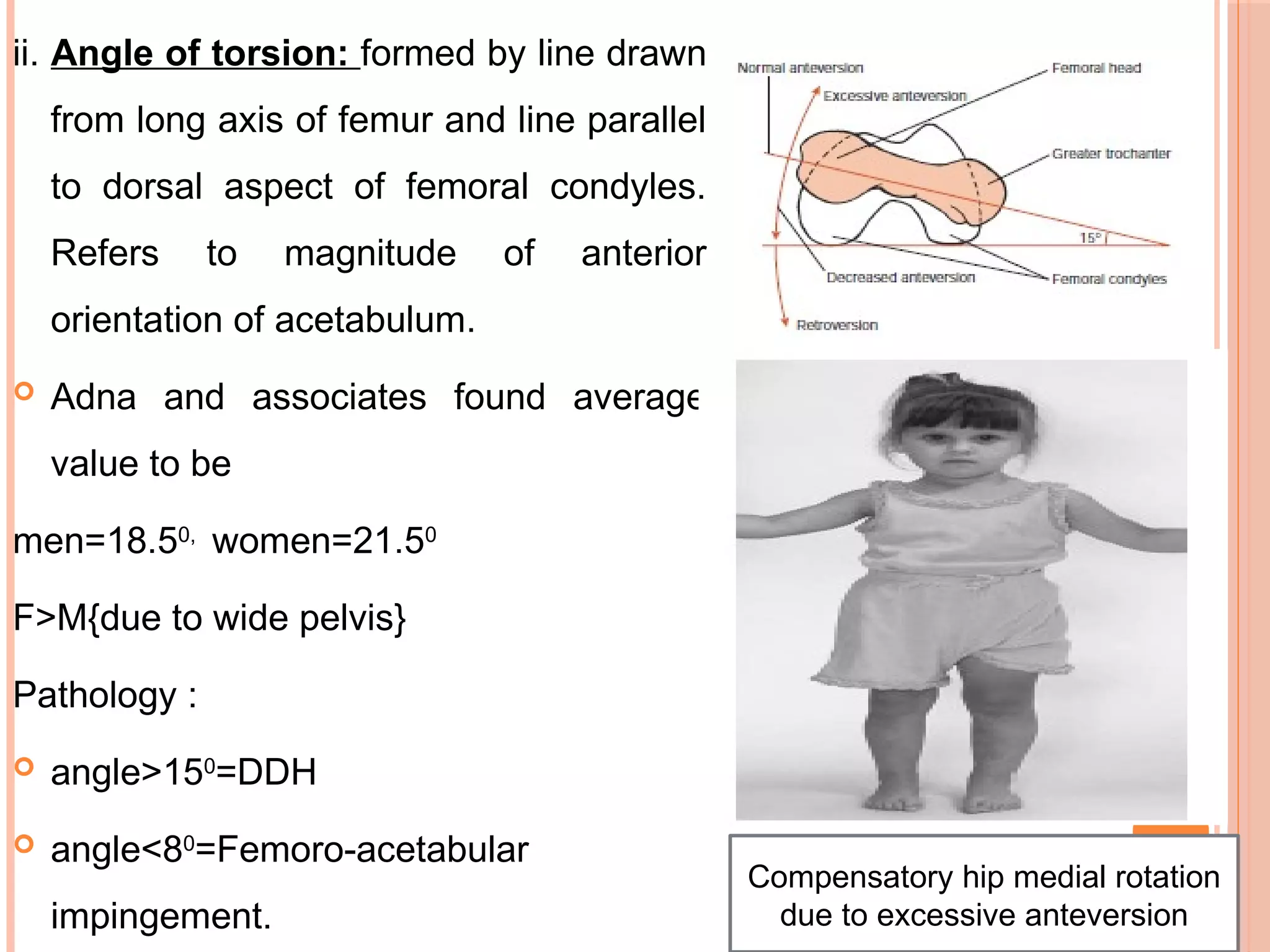
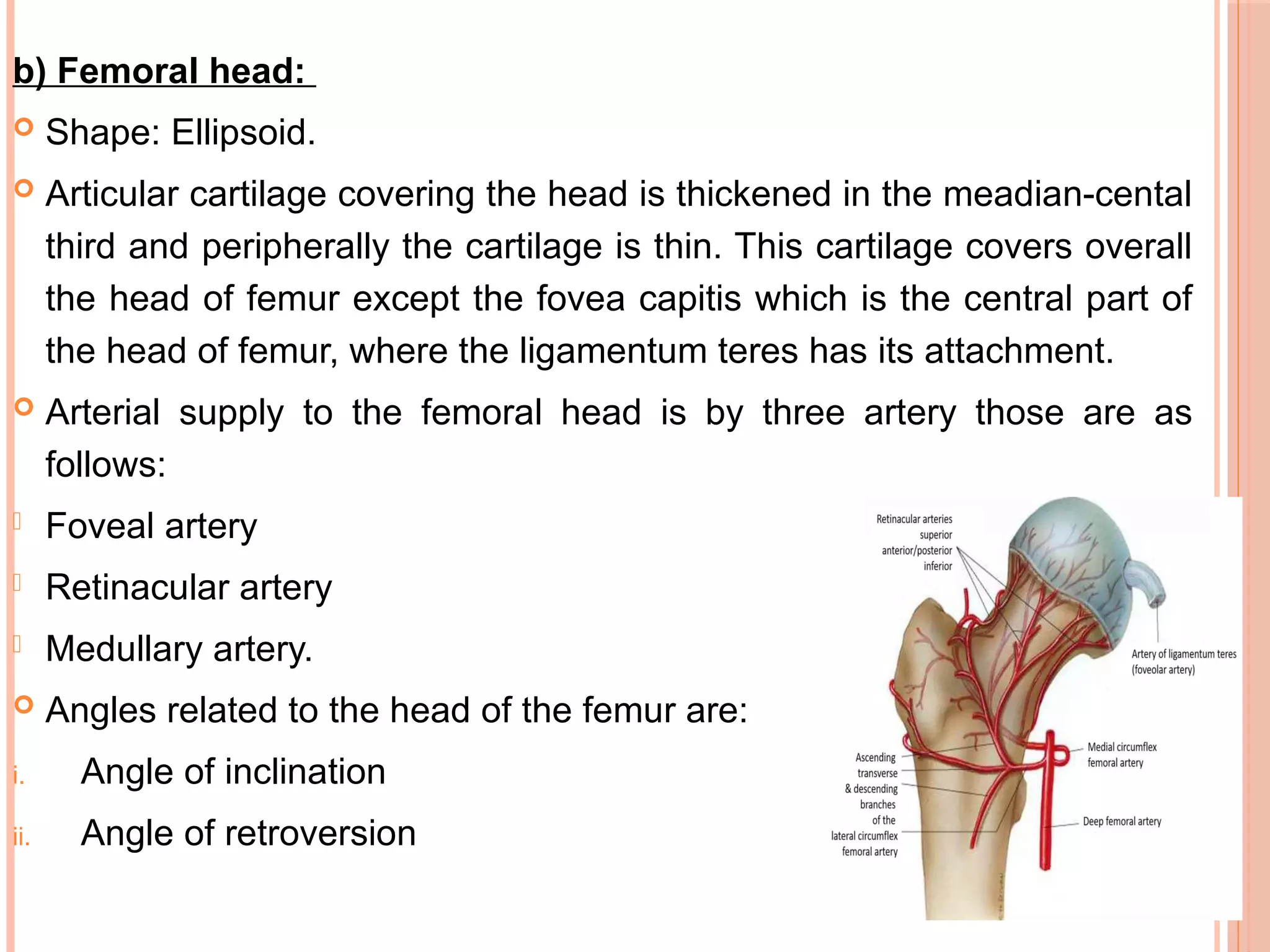
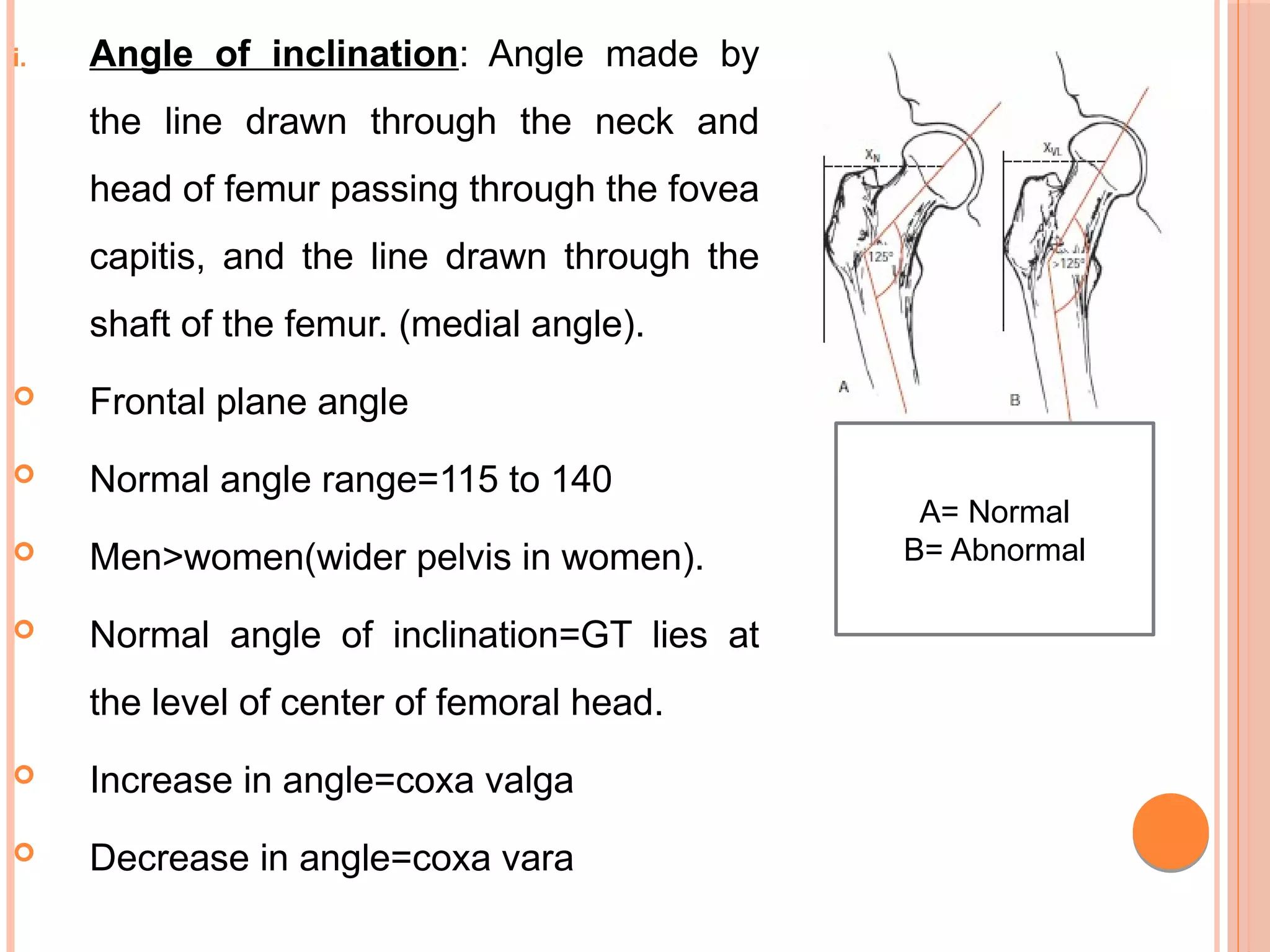
The document discusses the anatomy and biomechanics of the hip joint. It describes the ball and socket structure of the hip joint formed by the acetabulum and femoral head. It details the angles of the hip joint including the central edge angle and angle of anteversion. It discusses the muscles, ligaments, biomechanics including ranges of motion, and forces across the hip joint during activities like standing, walking, and squatting. Pathomechanics of conditions like hip fractures and dislocations are also mentioned.























































































