Downloaded 114 times
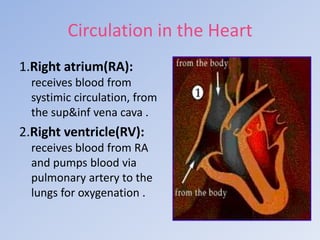
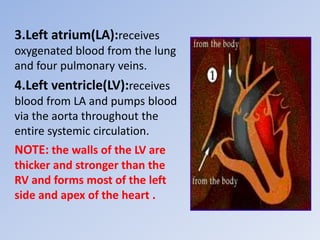
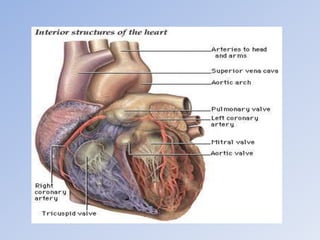
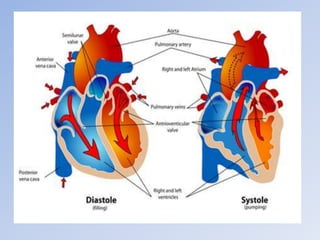
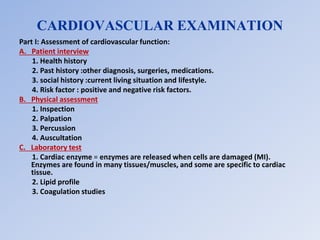

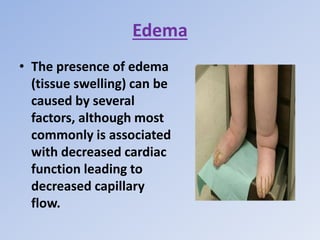
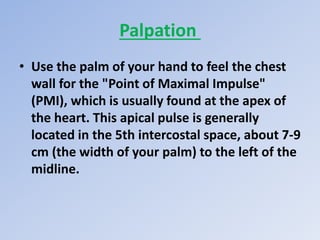
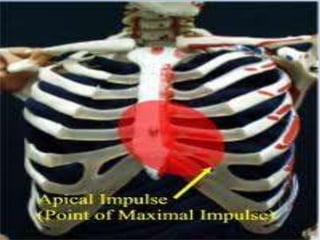



This document provides an overview of cardiovascular assessment. It begins by outlining the objectives of reviewing cardiovascular anatomy and physiology, physical assessment techniques, and diagnostic procedures. It then describes the anatomy of the heart, including its four chambers and valves. Physical assessment techniques are explained, including inspection, palpation, percussion, and auscultation to evaluate the heart sounds and pulses. Common diagnostic tests like electrocardiograms, stress tests, and cardiac catheterization are also briefly mentioned.