
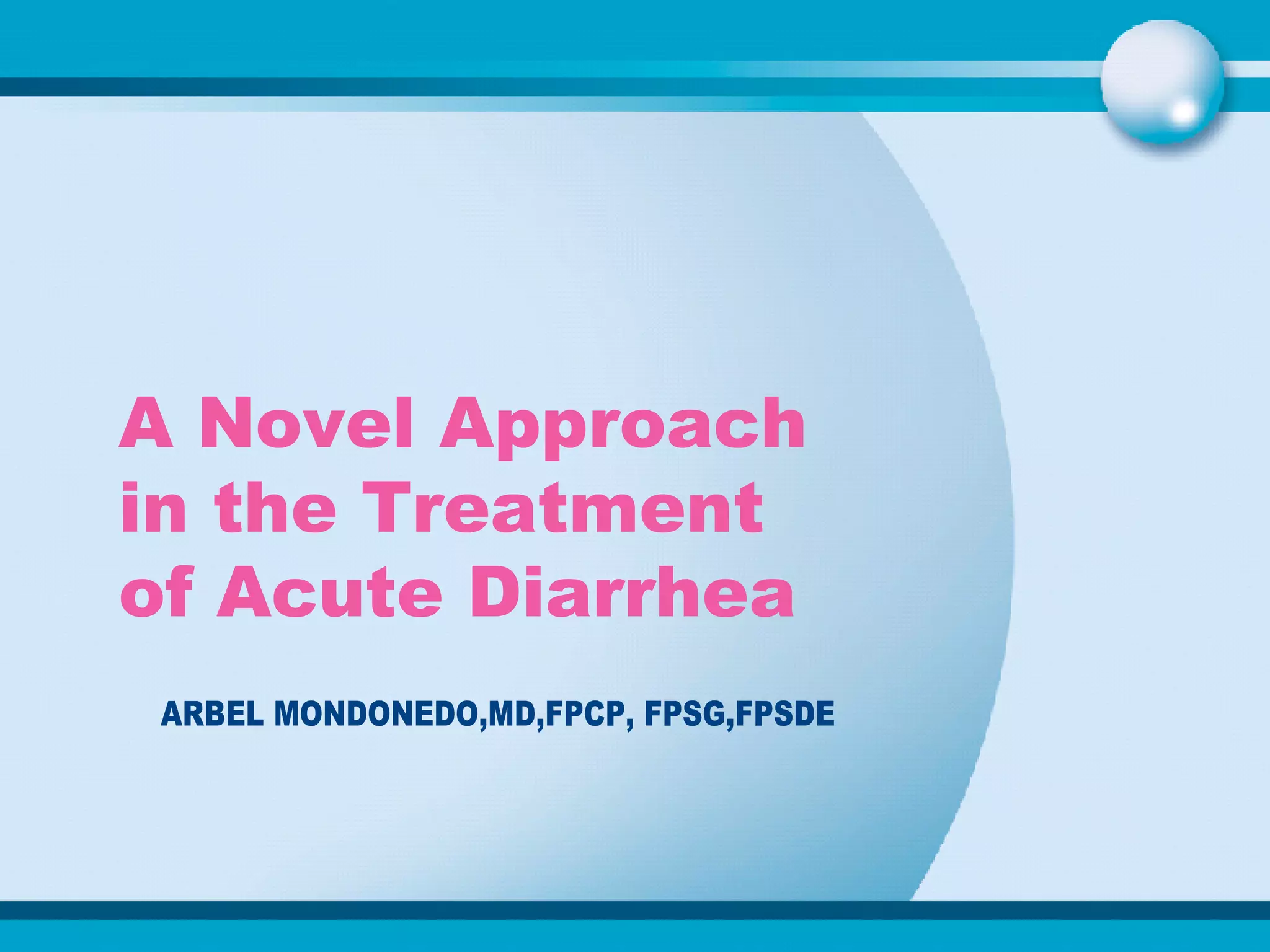

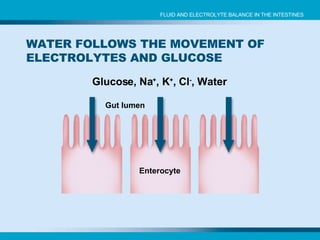
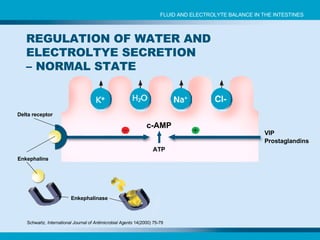

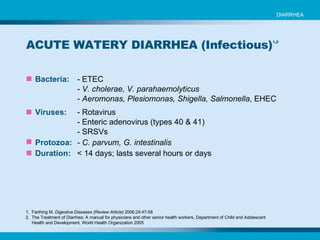
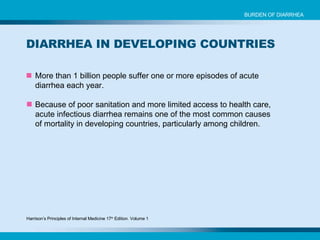



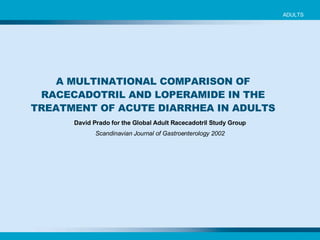
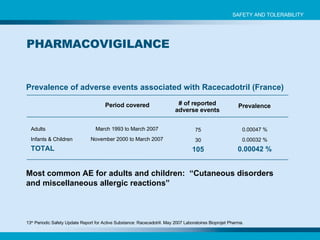
![Characteristics of population at inclusion Age [months] 13 12 Weight [kg] 9.0 8.7 Duration of diarrhea before inclusion [hrs] 47.4 51.5 Stool number in the last 24 hours 8.6 9.7 Stool consistency [no. of boys] Loose 16 14 Watery 52 53 Characteristic Racecadotril + ORS Placebo + ORS [ n = 68] [n = 67] Salazar-Lindo E, Santisteban-Ponce J, Chea-Wood E and Guterriez M. N Engl J Med 2000;343:463-467 RACECADOTRIL IN THE TREATMENT OF ACUTE WATERY DIARRHEA IN CHILDREN (Salazar-Lindo et al.) INFANTS AND CHILDREN](https://image.slidesharecdn.com/hidrasec-bongs-lecture-1197279973313586-3/85/Hidrasec-Bongs-Lecture-46-320.jpg)
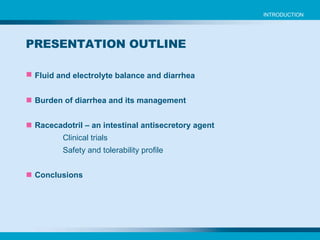
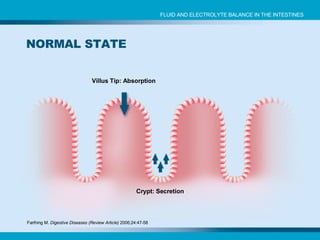
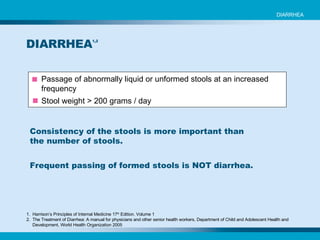
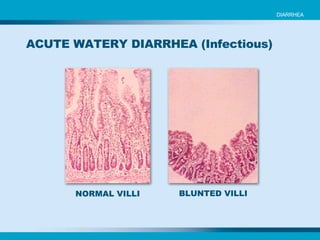
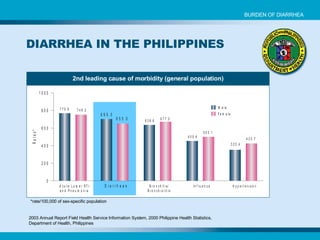
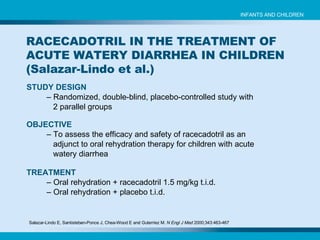
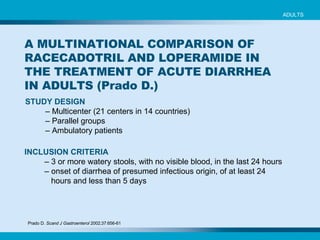
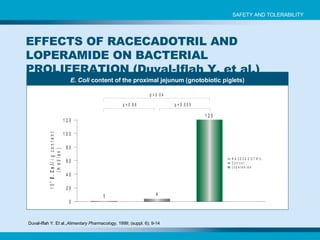
![Characteristics of population at inclusion CHARACTERISTIC Racecadotril + ORS Placebo + ORS [n = 84] [n = 82] Age [months] 12.0 ± 0.9 13.6 ± 1.0 Sex: [M / F] 51 / 38 50 / 33 Height [m] 0.73 ± 0.01 0.75 ± 0.01 Weight [kg] 8.54 ± 0.25 9.27 ± 0.25 Stool number [n] 6.0 ± 0.3 6.5 ± 0.4 Duration of diarrhea [days] 2.0 ± 0.2 1.9 ± 0.1 Patients with Rotavirus [n] 32 35 Patients with Adenovirus [n] 3 4 Mean + SEM Cézard JP et al. Gastroenterology 2001;120:799-805. EFFICACY AND TOLERABILITY OF RACECADOTRIL IN ACUTE DIARRHEA IN CHILDREN ( Cézard et al.) INFANTS AND CHILDREN](https://image.slidesharecdn.com/hidrasec-bongs-lecture-1197279973313586-3/85/Hidrasec-Bongs-Lecture-56-320.jpg)
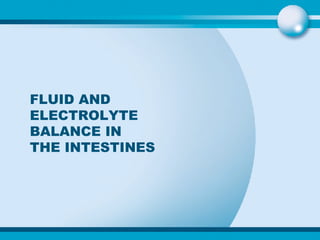
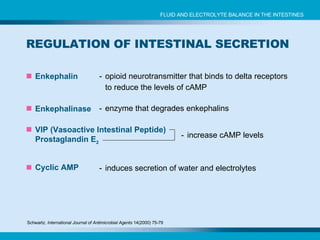
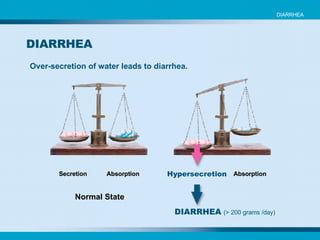
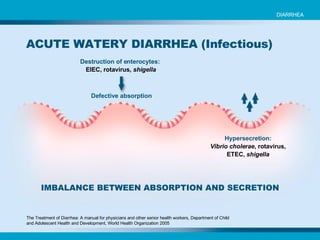
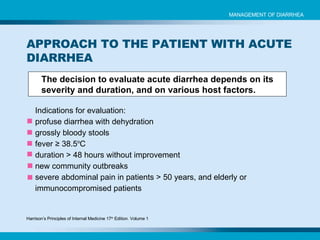
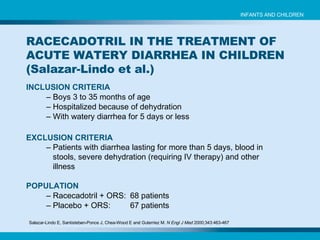
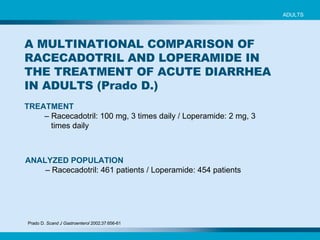
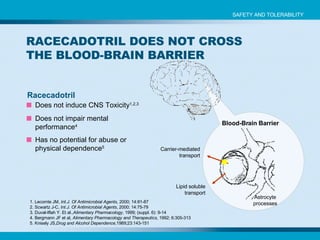
![Time to recovery in rotavirus-positive patients Cézard JP et al. Gastroenterology 2001;120:799-805. EFFICACY AND TOLERABILITY OF RACECADOTRIL IN ACUTE DIARRHEA IN CHILDREN ( Cézard et al.) INFANTS AND CHILDREN Duration of diarrhea [median, hours] Racecadotril [n = 32] Placebo [n = 35] P 6.9 36 0.02](https://image.slidesharecdn.com/hidrasec-bongs-lecture-1197279973313586-3/85/Hidrasec-Bongs-Lecture-58-320.jpg)

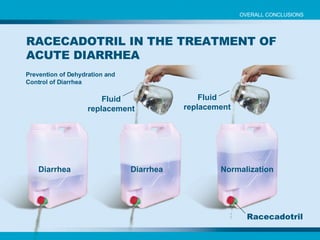
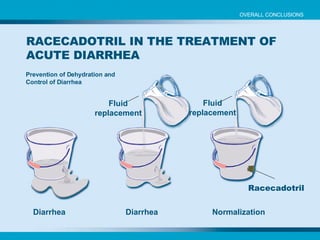

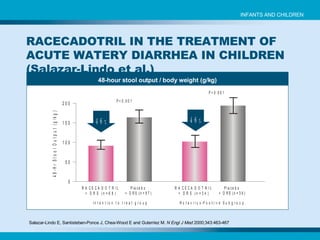
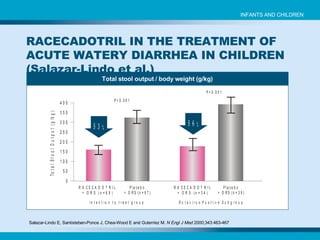
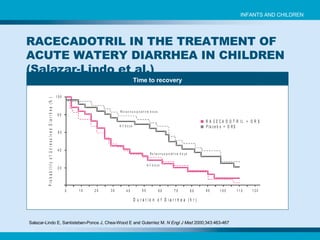
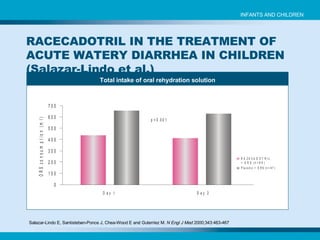
This document summarizes a clinical trial that evaluated the efficacy and safety of racecadotril for treating acute watery diarrhea in children. The randomized, double-blind, placebo-controlled trial found that racecadotril significantly reduced stool output in children over 48 hours compared to the placebo group receiving only oral rehydration therapy. Racecadotril was well-tolerated with few adverse effects reported. The study provides evidence that racecadotril is an effective adjunct treatment to oral rehydration for managing acute watery diarrhea in children.























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













