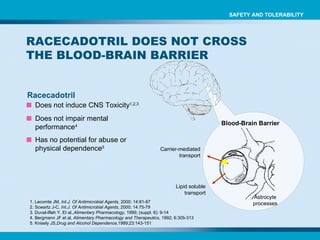
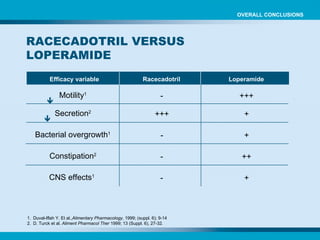
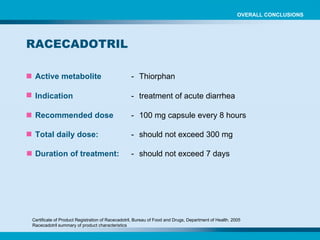
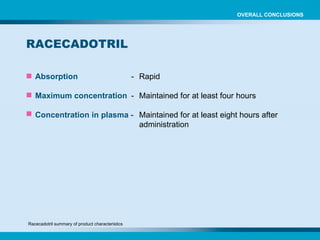
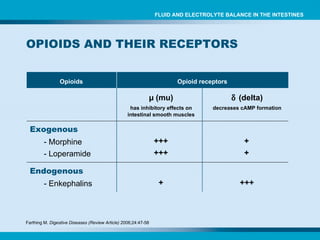
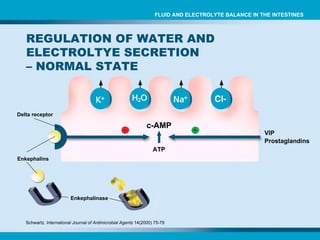
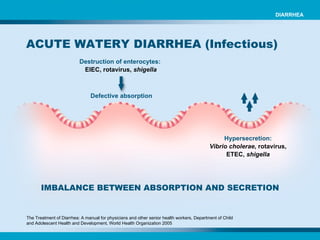
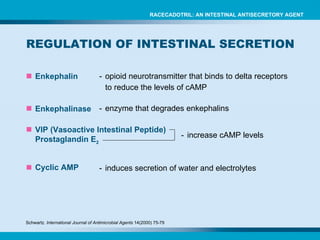
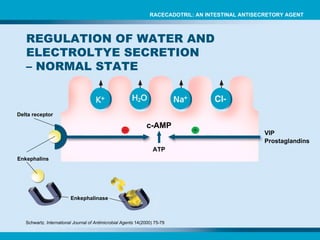
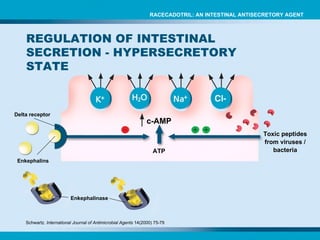
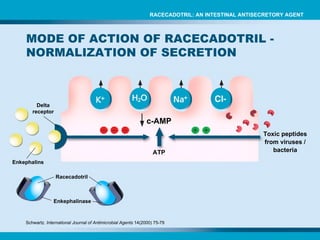
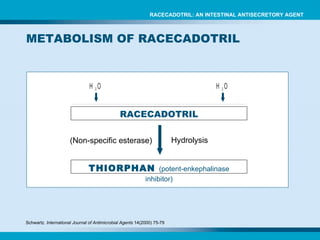
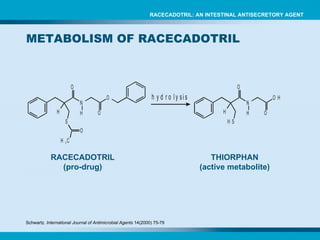
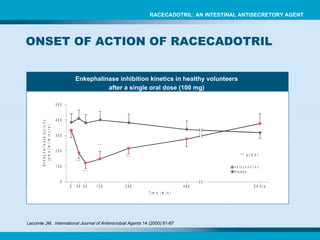
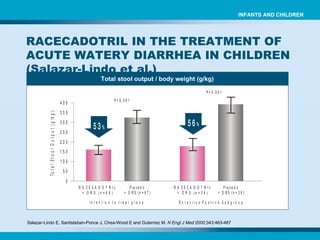
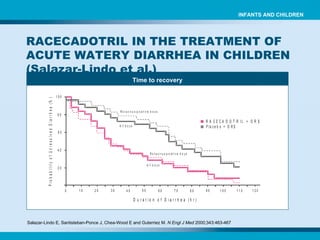
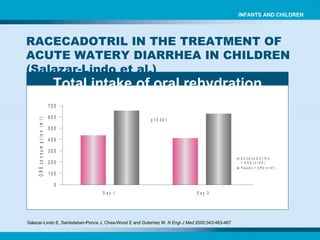
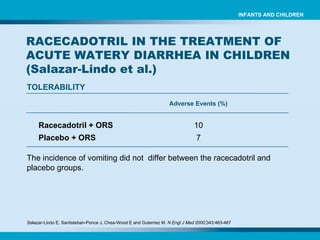
Racecadotril is an intestinal antisecretory agent that inhibits intestinal fluid secretion. It works by inhibiting the enzyme enkephalinase, which breaks down the endogenous opioid peptide enkephalin. Enkephalin binds to delta receptors on intestinal cells and reduces cyclic AMP formation, thereby decreasing intestinal fluid secretion. Clinical trials have shown that racecadotril reduces stool output and shortens the time to recovery in children with acute watery diarrhea when used as an adjunct to oral rehydration therapy. It provides benefits over current diarrhea treatments by inhibiting intestinal hypersecretion while having a rapid onset, limited constipating effects, and good safety profile.



![Time to recovery in rotavirus-positive patients Cézard JP et al. Gastroenterology 2001;120:799-805. EFFICACY AND TOLERABILITY OF RACECADOTRIL IN ACUTE DIARRHEA IN CHILDREN ( Cézard et al.) INFANTS AND CHILDREN Duration of diarrhea [median, hours] Racecadotril [n = 32] Placebo [n = 35] P 6.9 36 0.02](https://image.slidesharecdn.com/9852514-1233950395778127-1/85/racecadotril-56-320.jpg)