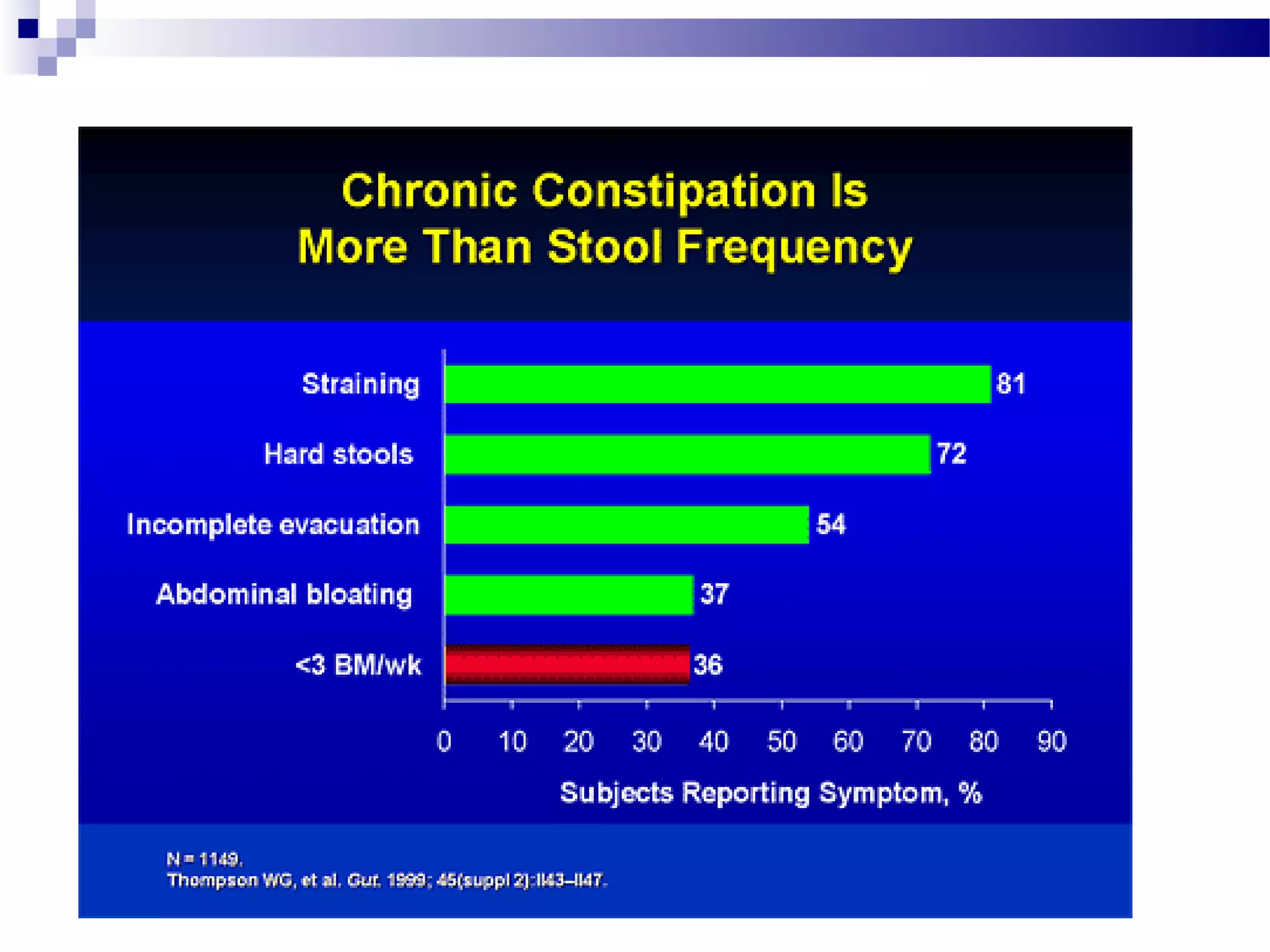
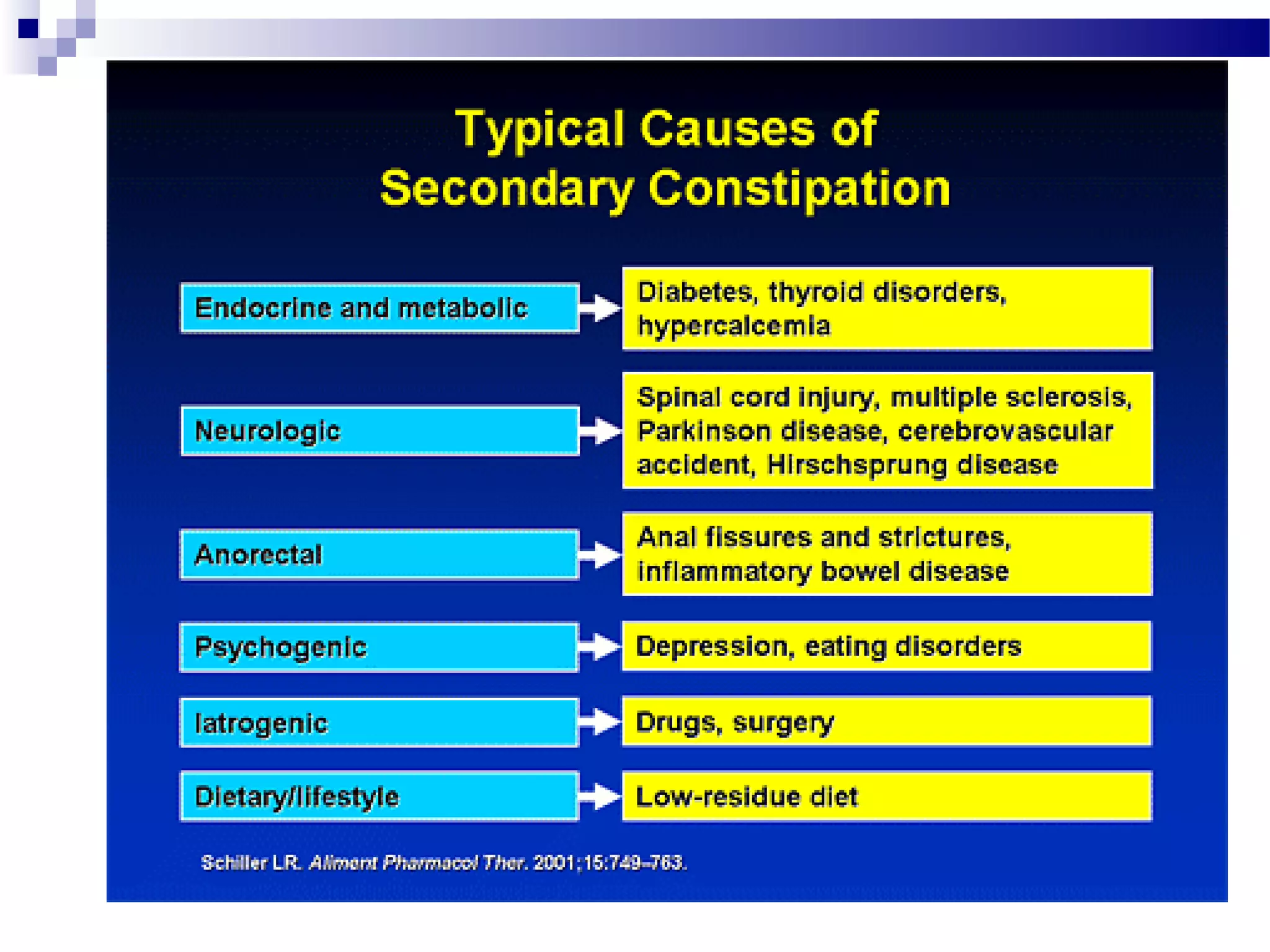
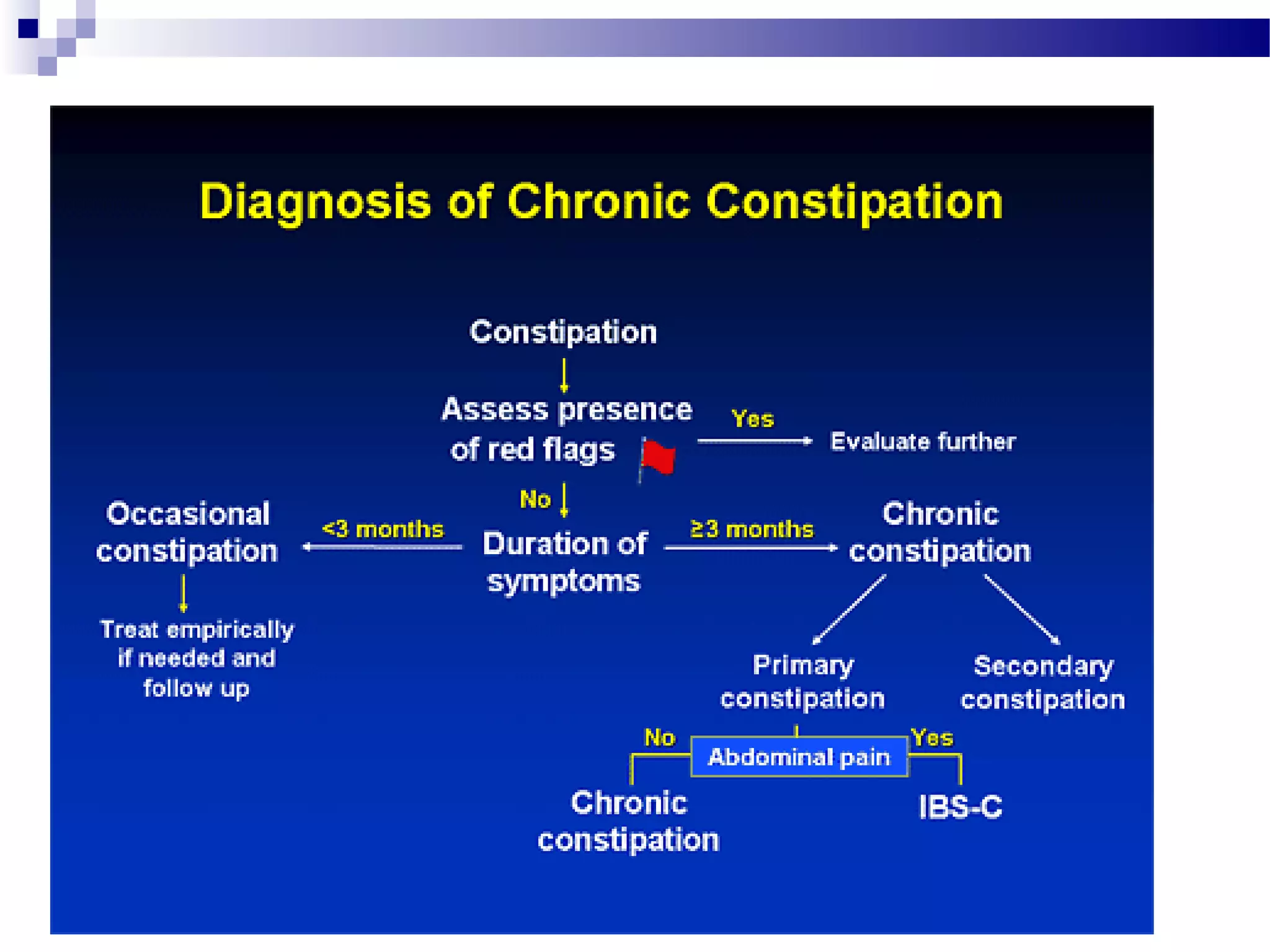
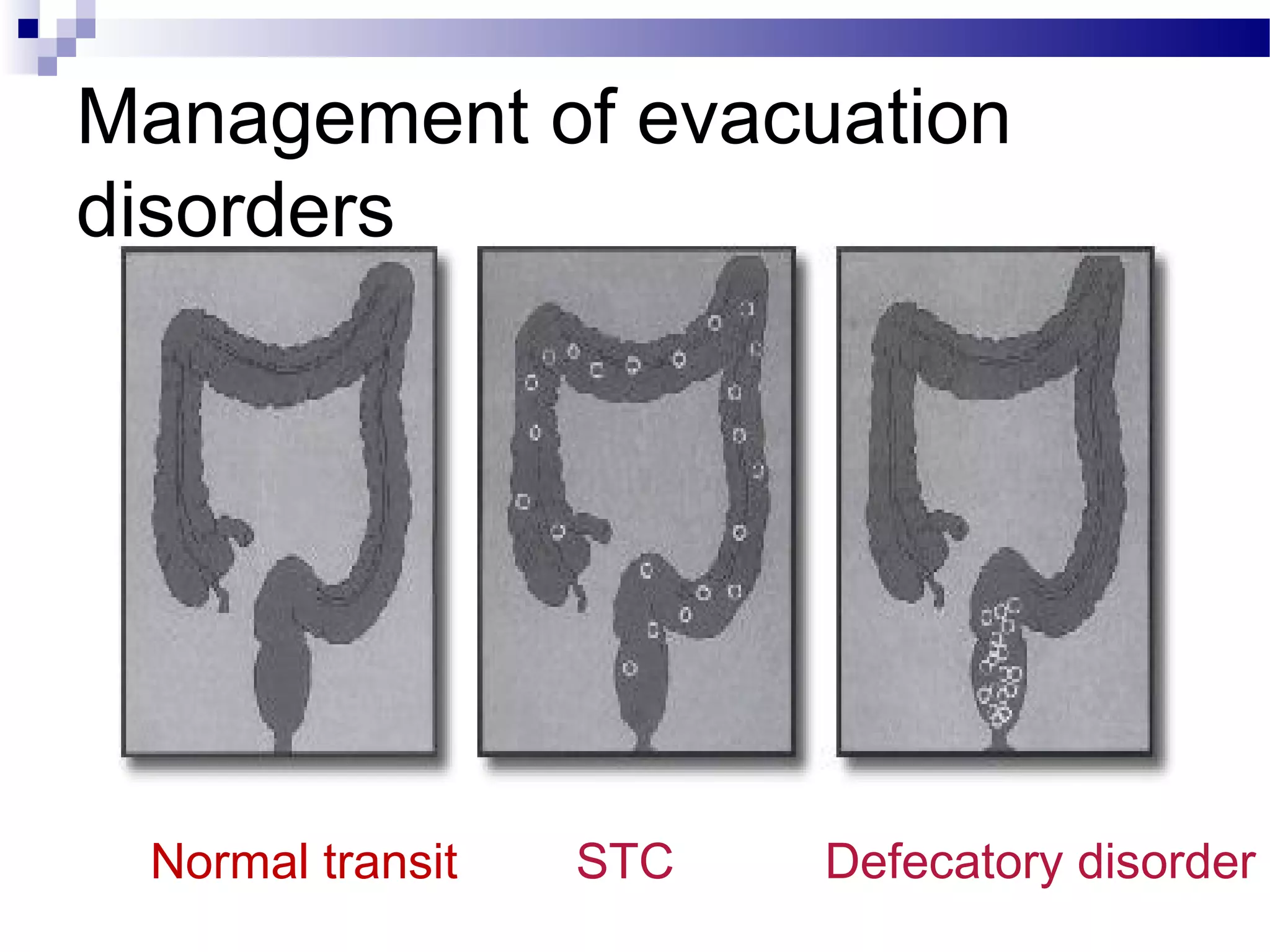
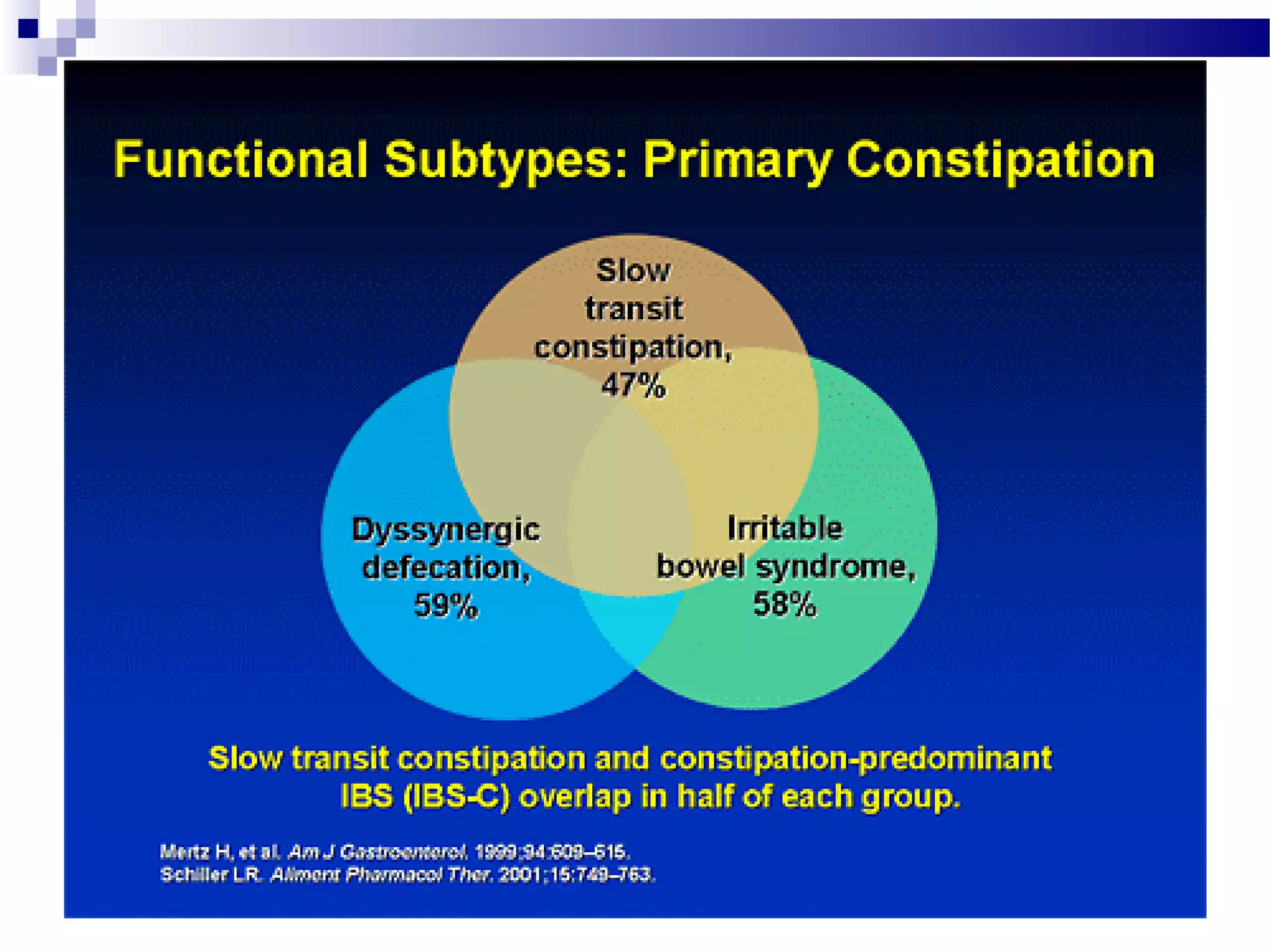
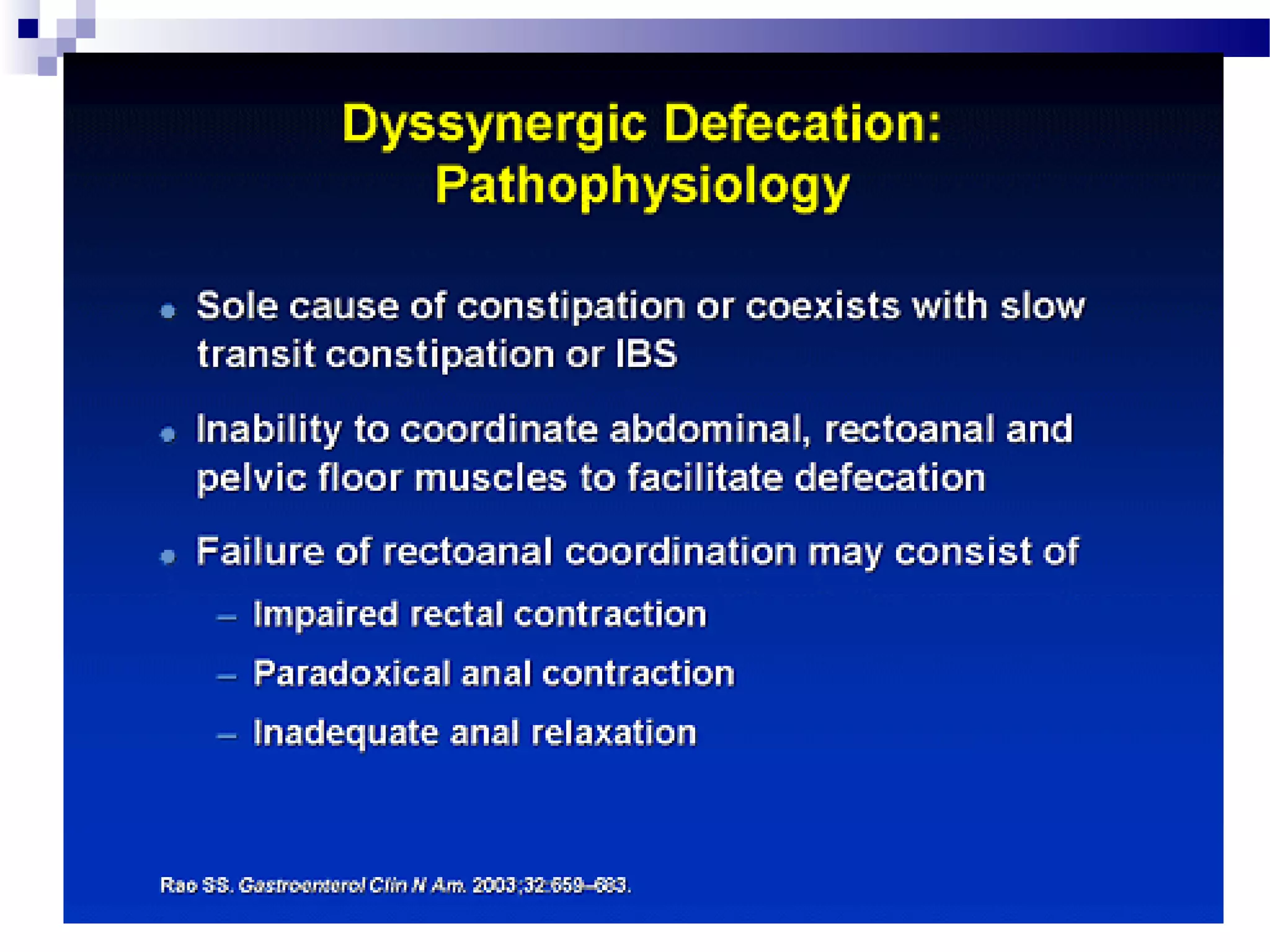
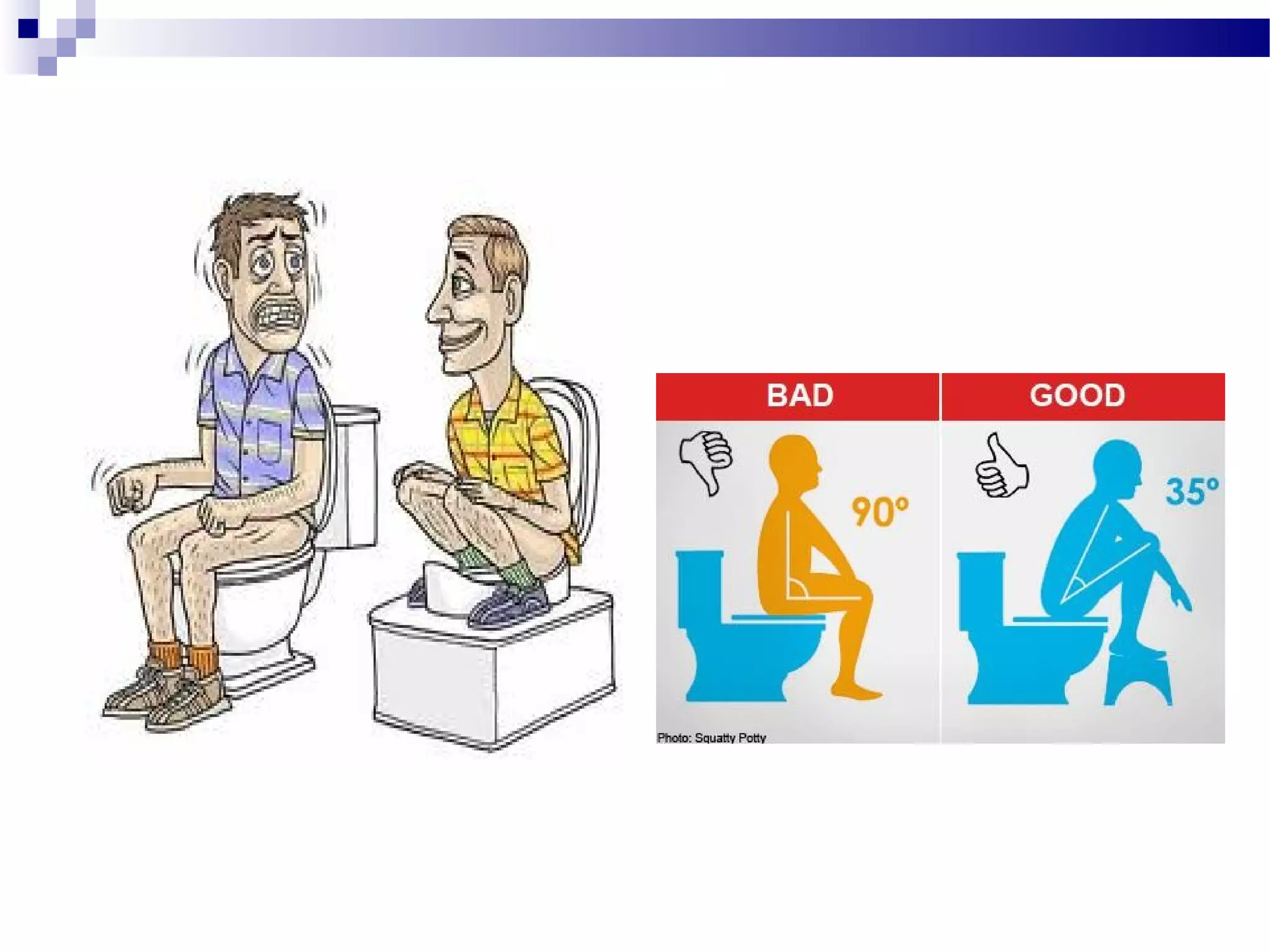
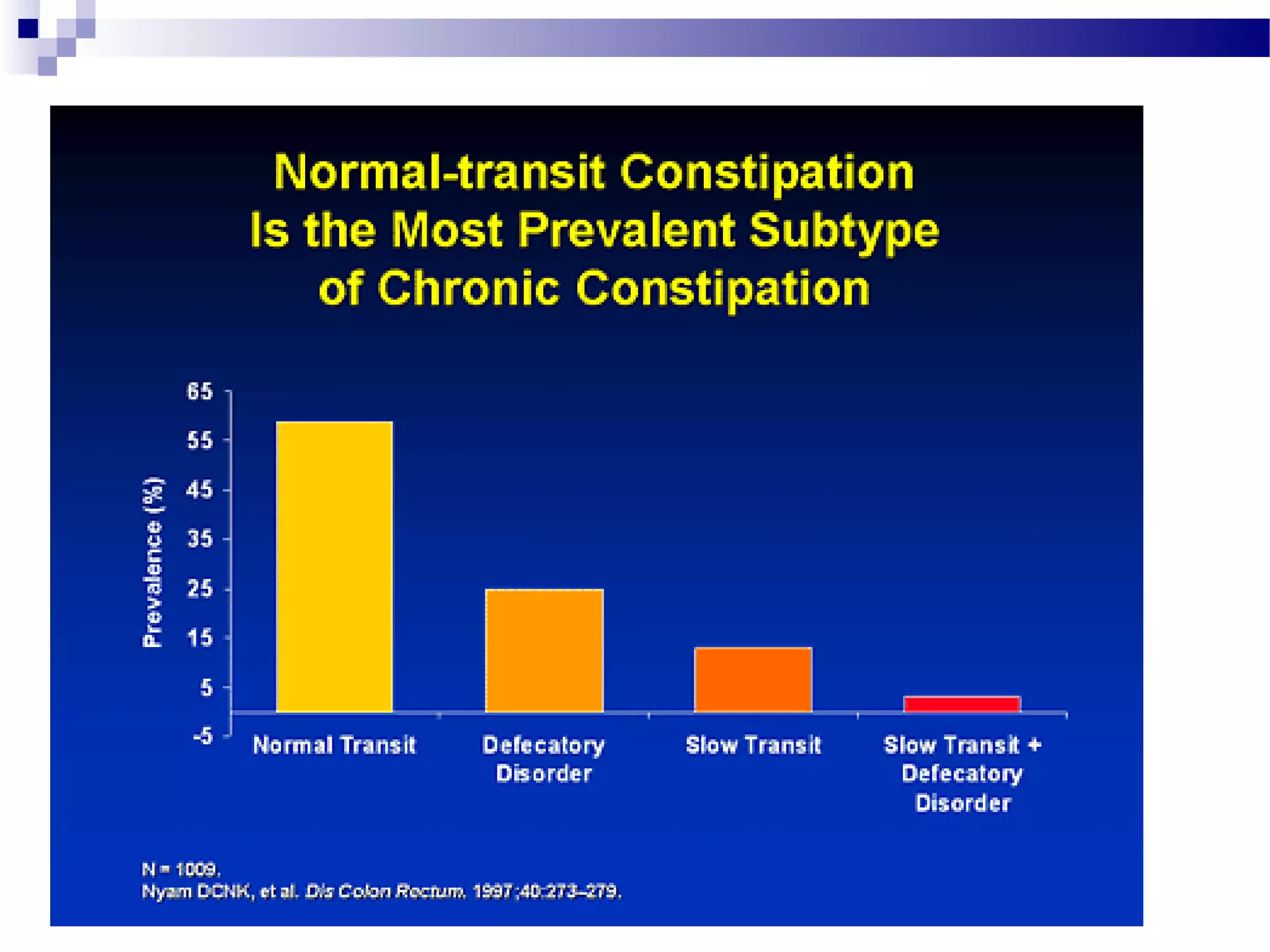
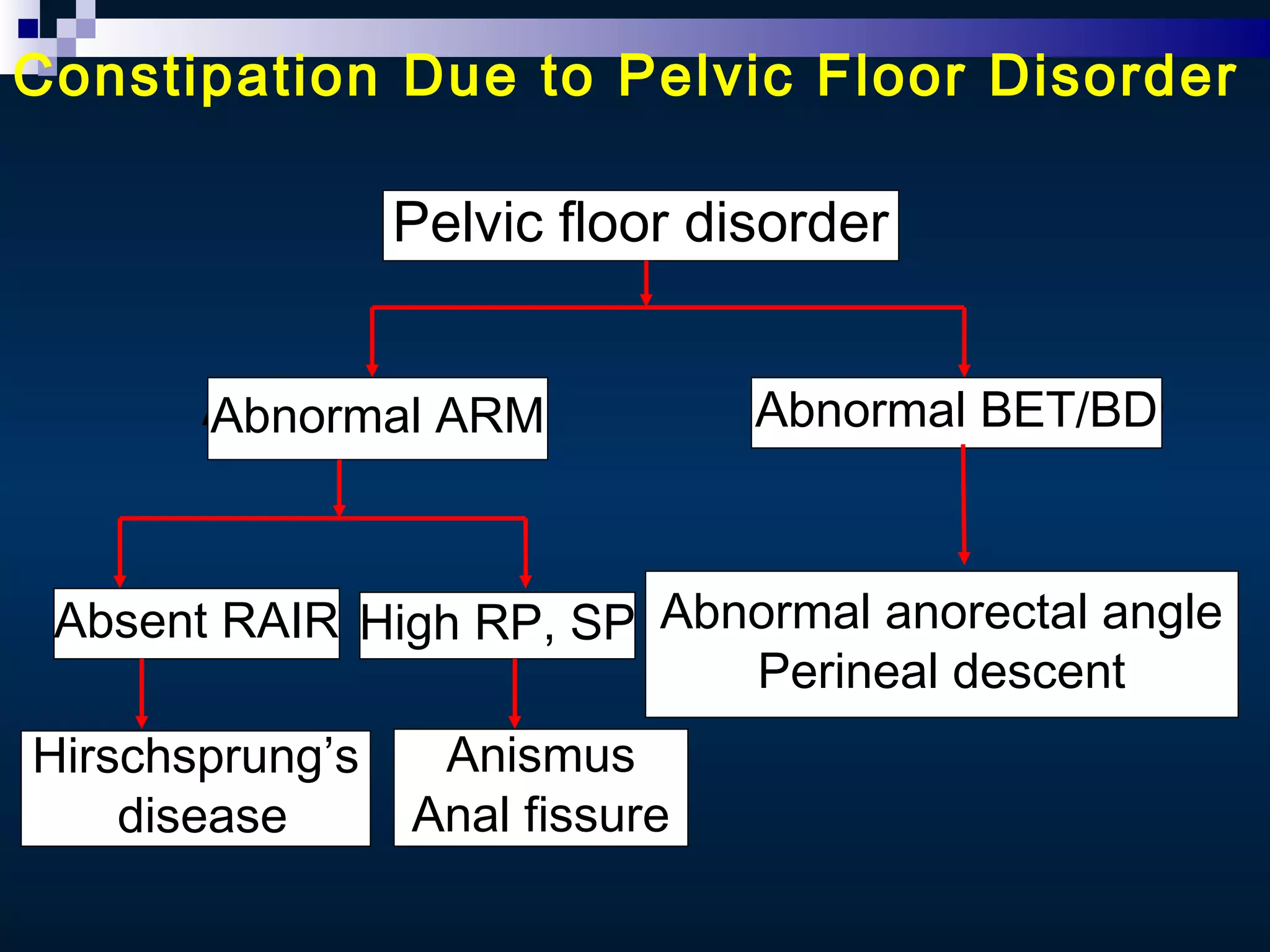
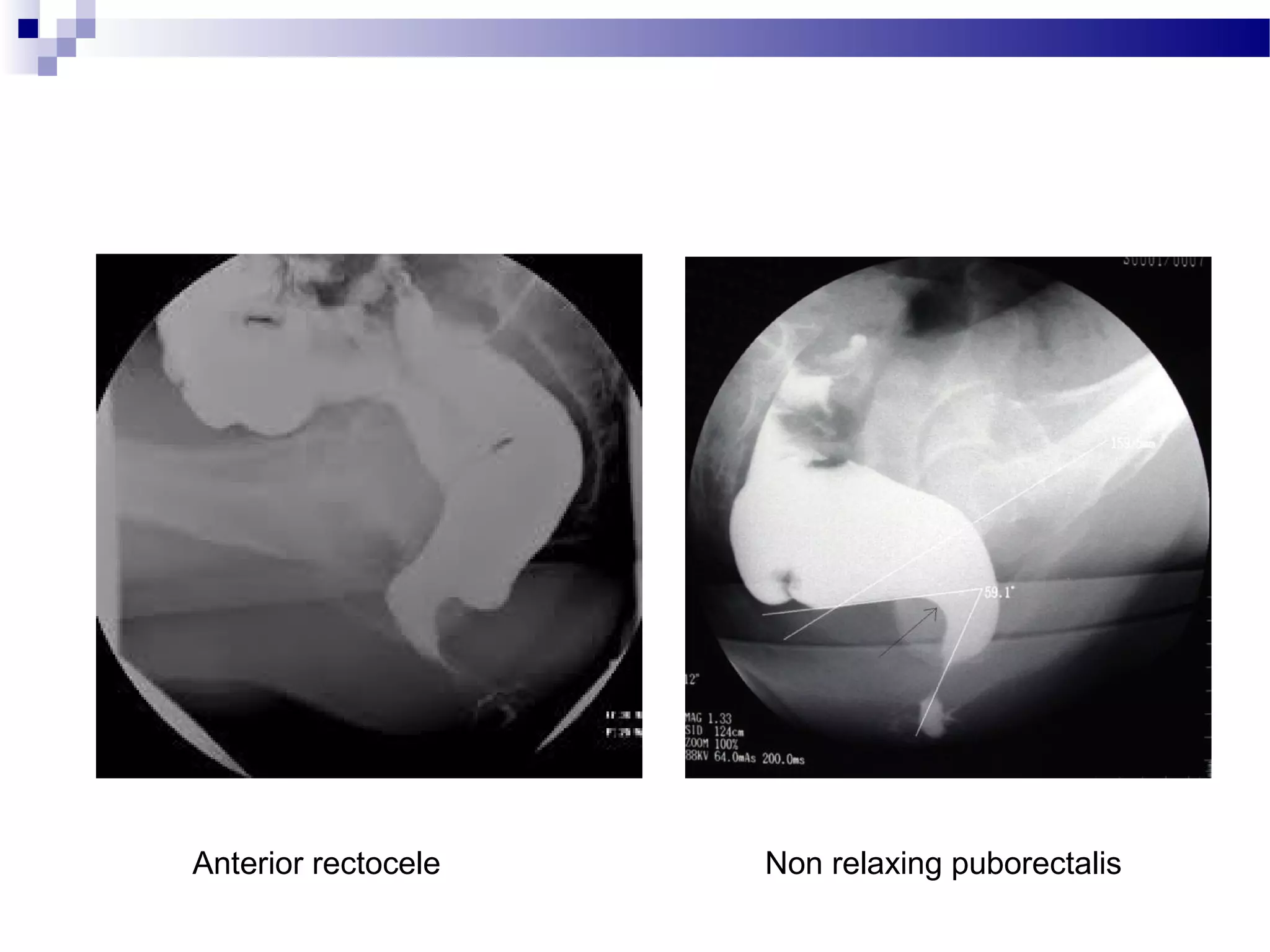
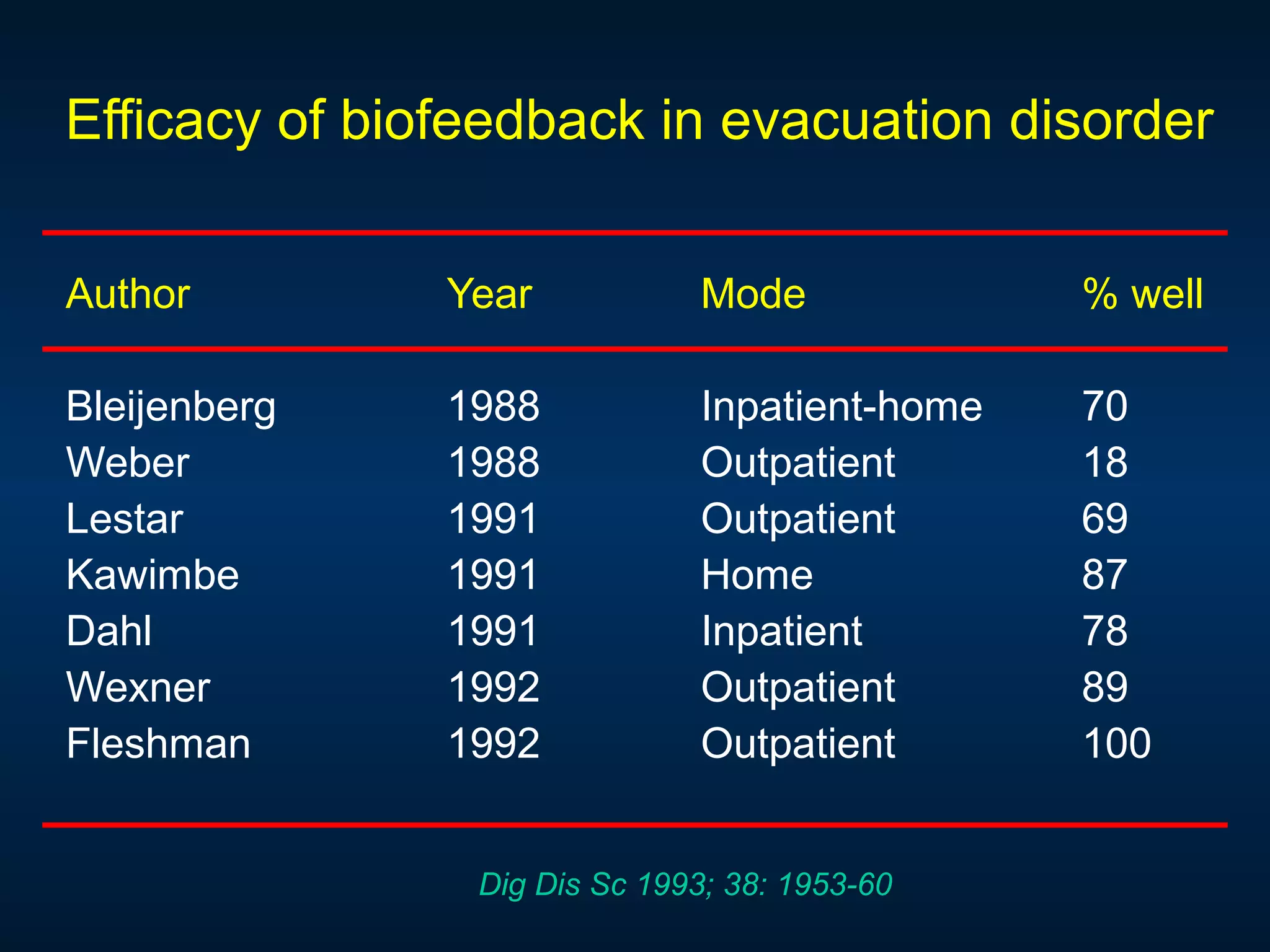
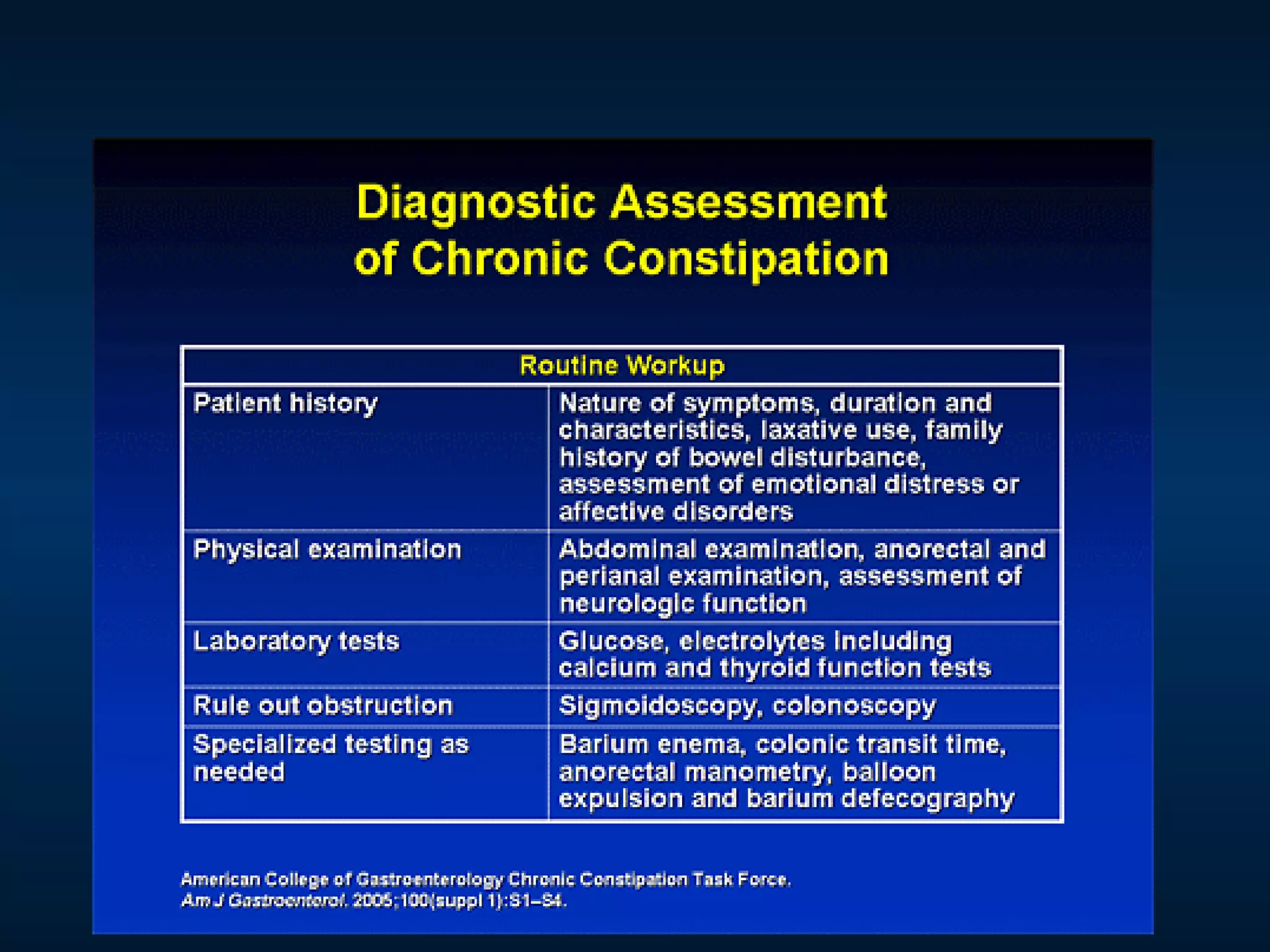
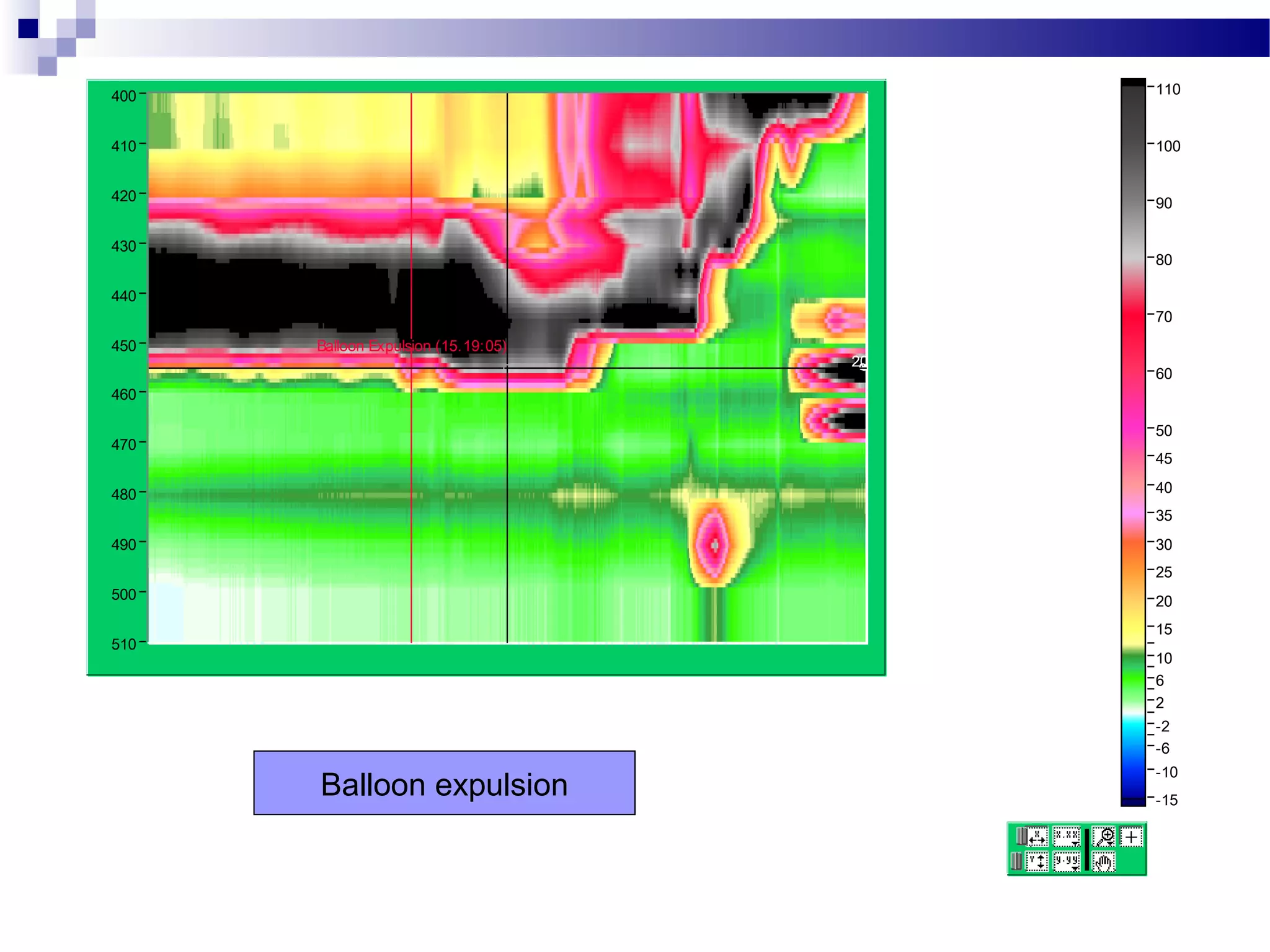
The document discusses the evaluation and management of constipation. It outlines the clinical approach which includes determining if it is constipation, identifying potential causes like drugs or disease, and checking for alarm symptoms. Evaluation involves examination, labs like TSH and calcium, and tests like anorectal manometry and balloon expulsion tests to classify constipation and identify defecatory disorders. Biofeedback therapy is described as the treatment of choice for defecatory disorders by training muscles through visual cues. Surgery may be considered for issues like rectocele or Hirschsprung's disease.