Downloaded 79 times

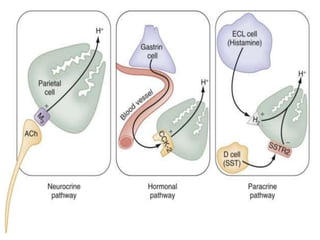
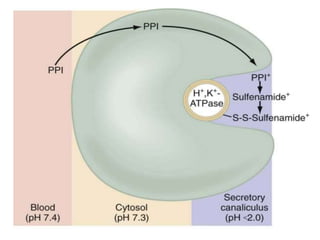
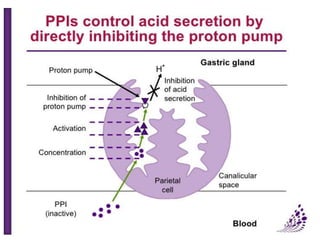
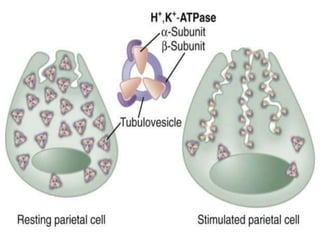
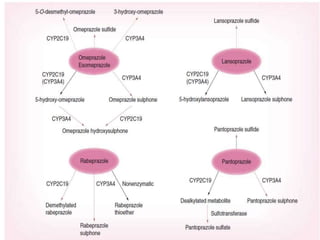
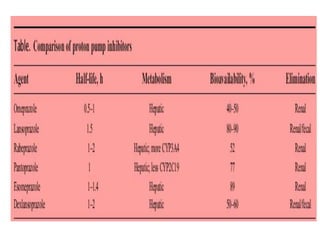
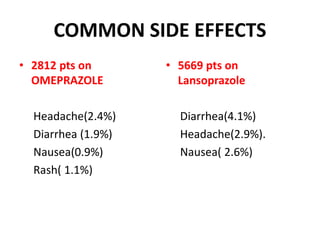
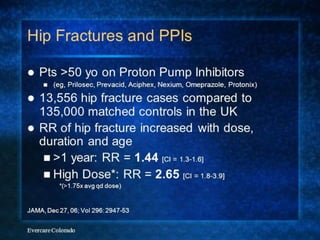

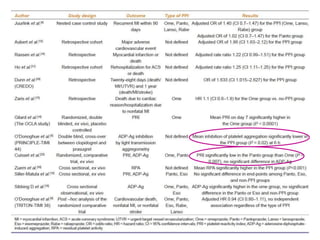


PPI's work by inhibiting gastric H+K+-ATPase and decreasing acid secretion. They are indicated for peptic ulcer disease, gastroesophageal reflux disease, and other acid-related conditions. Common side effects include diarrhea and headache. Long-term PPI use has been associated with nutrient deficiencies, increased risk of fractures, community-acquired pneumonia, and small intestinal bacterial overgrowth. PPIs also interact with some drugs by affecting CYP enzyme metabolism.