Downloaded 269 times


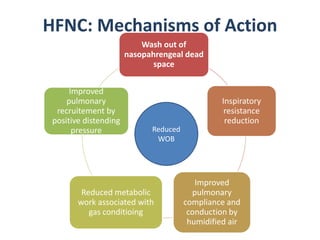
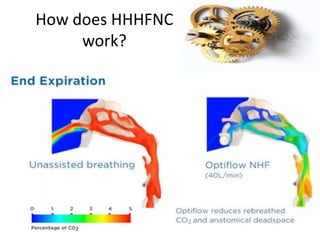
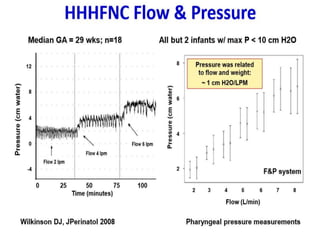
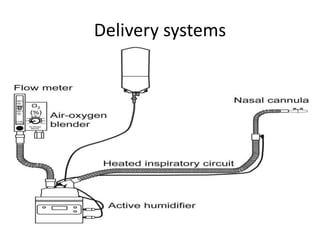




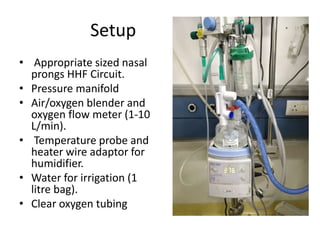
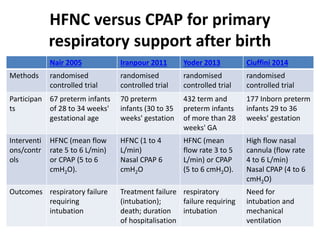
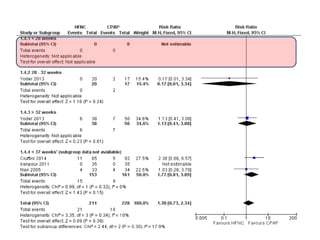
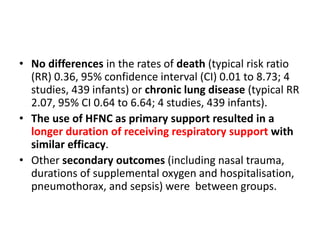
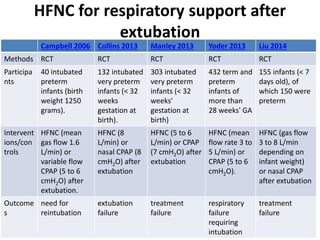
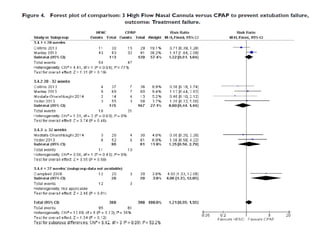

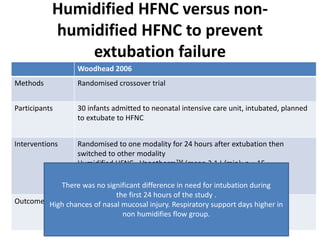
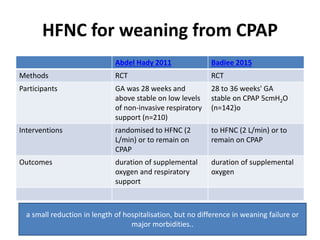
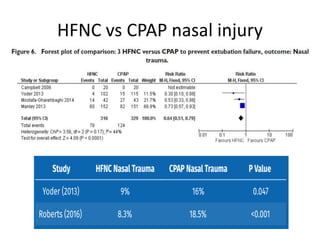
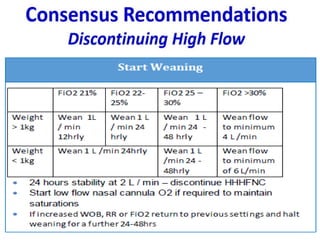


HFNC therapy is an alternative to CPAP for respiratory support of neonates. It works by flushing the nasal passages and removing exhaled gases, reducing dead space and resistance. HFNC provides a dynamic distending pressure of 3-5 cm H2O. It is indicated for mild respiratory dysfunction post-extubation or as an alternative to CPAP. Evidence shows HFNC has similar efficacy to CPAP with no differences in rates of reintubation, treatment failure, death or chronic lung disease when used for primary support or post-extubation. HFNC allows for a longer duration of non-invasive respiratory support.



































































