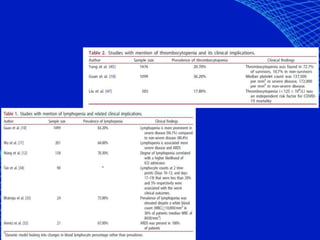
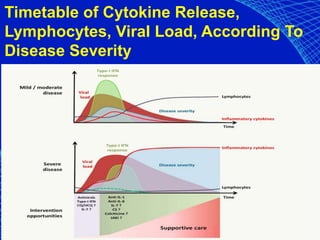
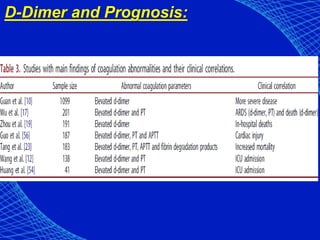
The document provides a comprehensive overview of the COVID-19 pandemic, detailing its virology, pathogenesis, symptoms, transmission, and the timeline of research and scientific publications related to the disease. It discusses the progression of infection, the impact of various treatments, and the vaccine development process while emphasizing the importance of high-quality research and peer review. Key findings include characteristics of the virus, modes of transmission, and treatment protocols, as well as the potential for reinfection and the role of coagulopathy in severe cases.


































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)