
Downloaded 23 times




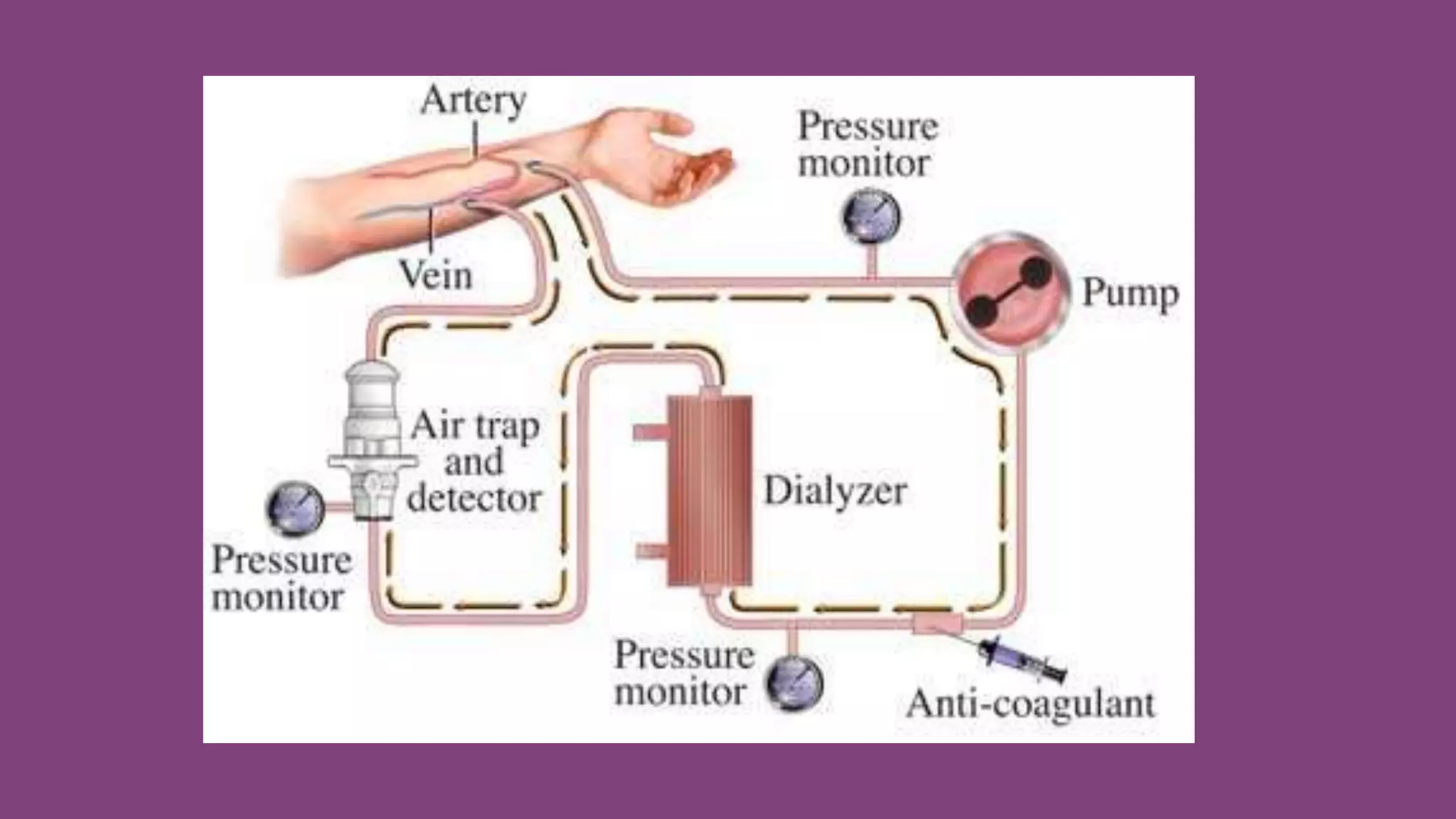








Hemodialysis is a process used to remove waste and excess fluid from the blood of patients with kidney failure. During hemodialysis, blood is pumped out of the body and into a dialyzer, where it passes through a semi-permeable membrane that removes toxins and fluid before returning clean blood to the body. Key aspects of hemodialysis include diffusion of wastes out of the blood, osmosis which removes excess water, and ultrafiltration of water under pressure. Patients typically require hemodialysis treatments lasting 4 hours, 3 times per week, either at a dialysis center or at home. Lifestyle management and monitoring for complications are important for patients on chronic hemodialysis























































































