Downloaded 325 times










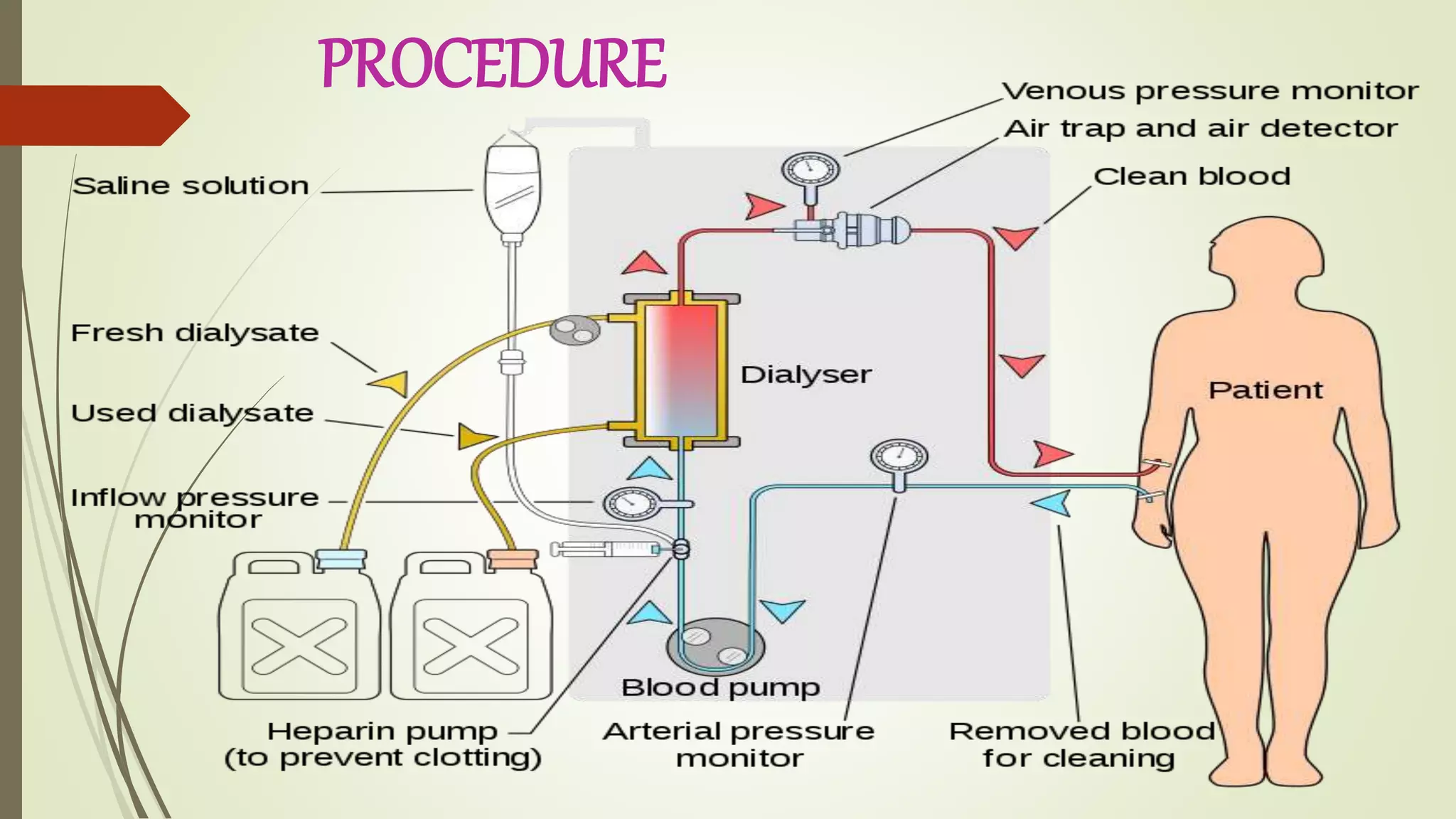




Hemodialysis is a medical procedure that uses a machine to filter waste and excess fluid from the blood of patients with kidney failure or injury. During hemodialysis, the patient's blood is pumped through a dialyzer filter to remove toxins and regulate electrolyte and mineral levels before being returned. It helps control symptoms but is not a cure for kidney disease. Vascular access is required, either through an arteriovenous fistula, graft, or temporary catheter placed in the subclavian, jugular, or femoral vein. Precise regulation of dialysate solutions, blood flow rates, and treatment time is needed to safely remove waste while avoiding complications.














































































