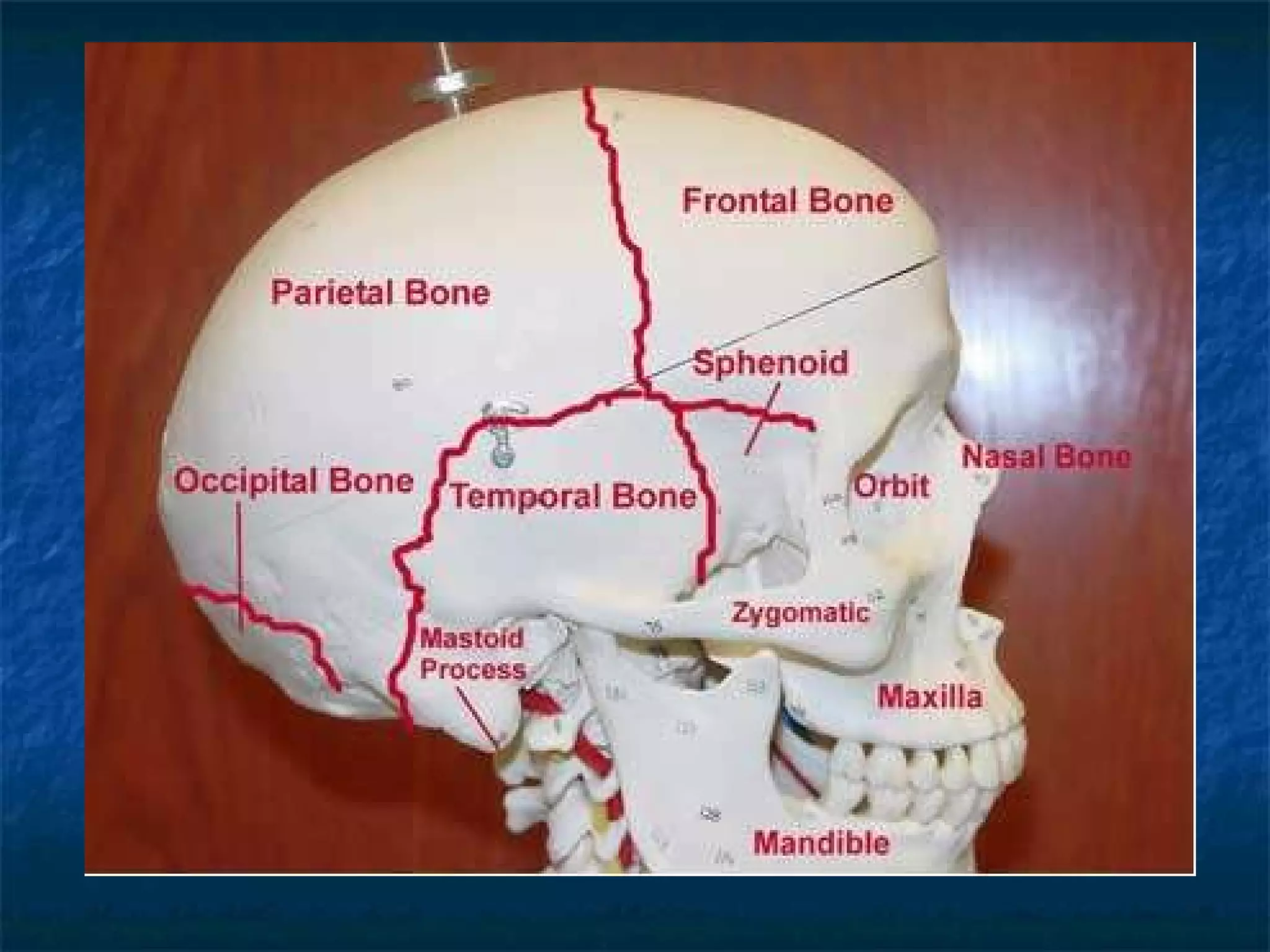
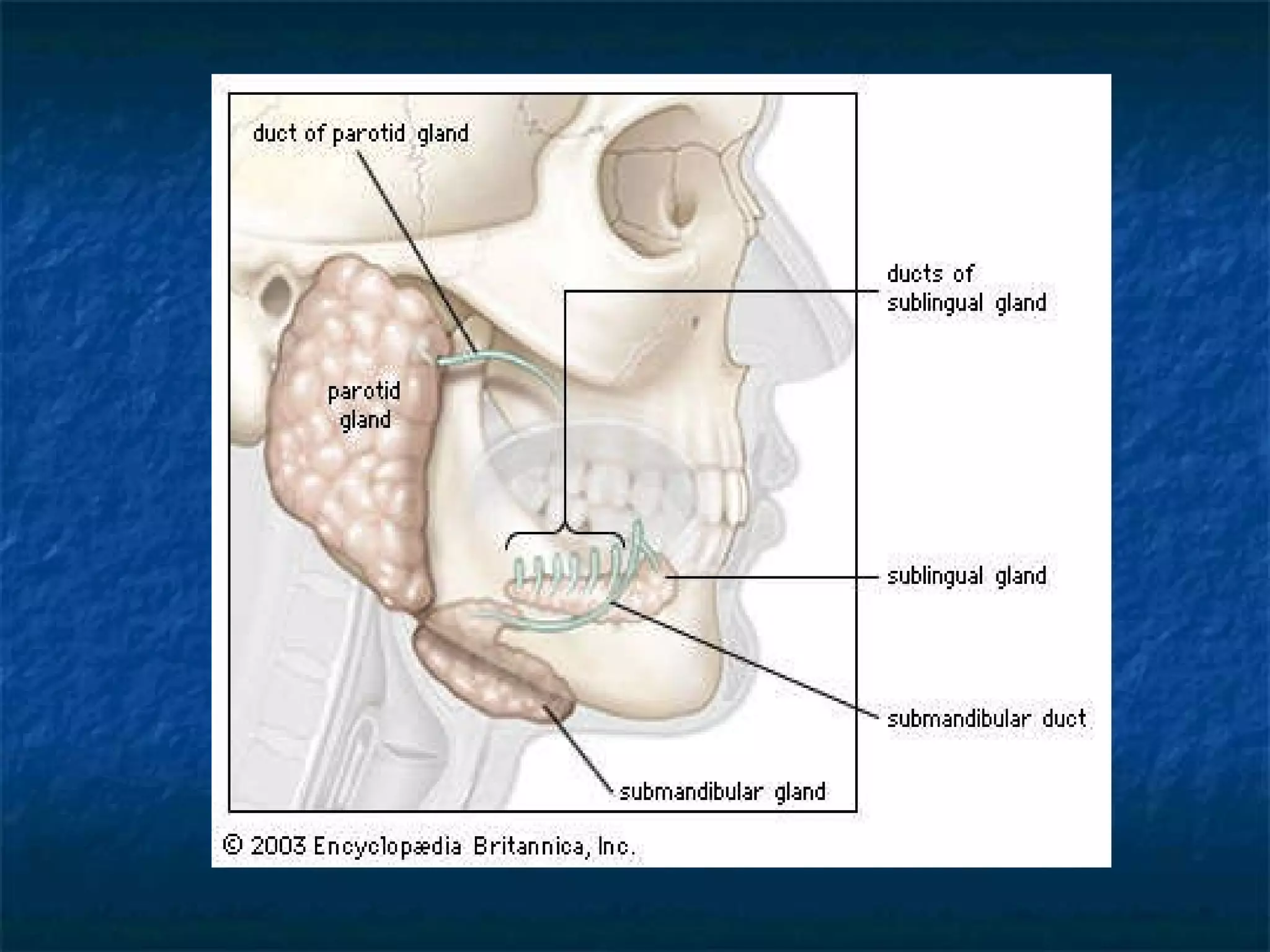
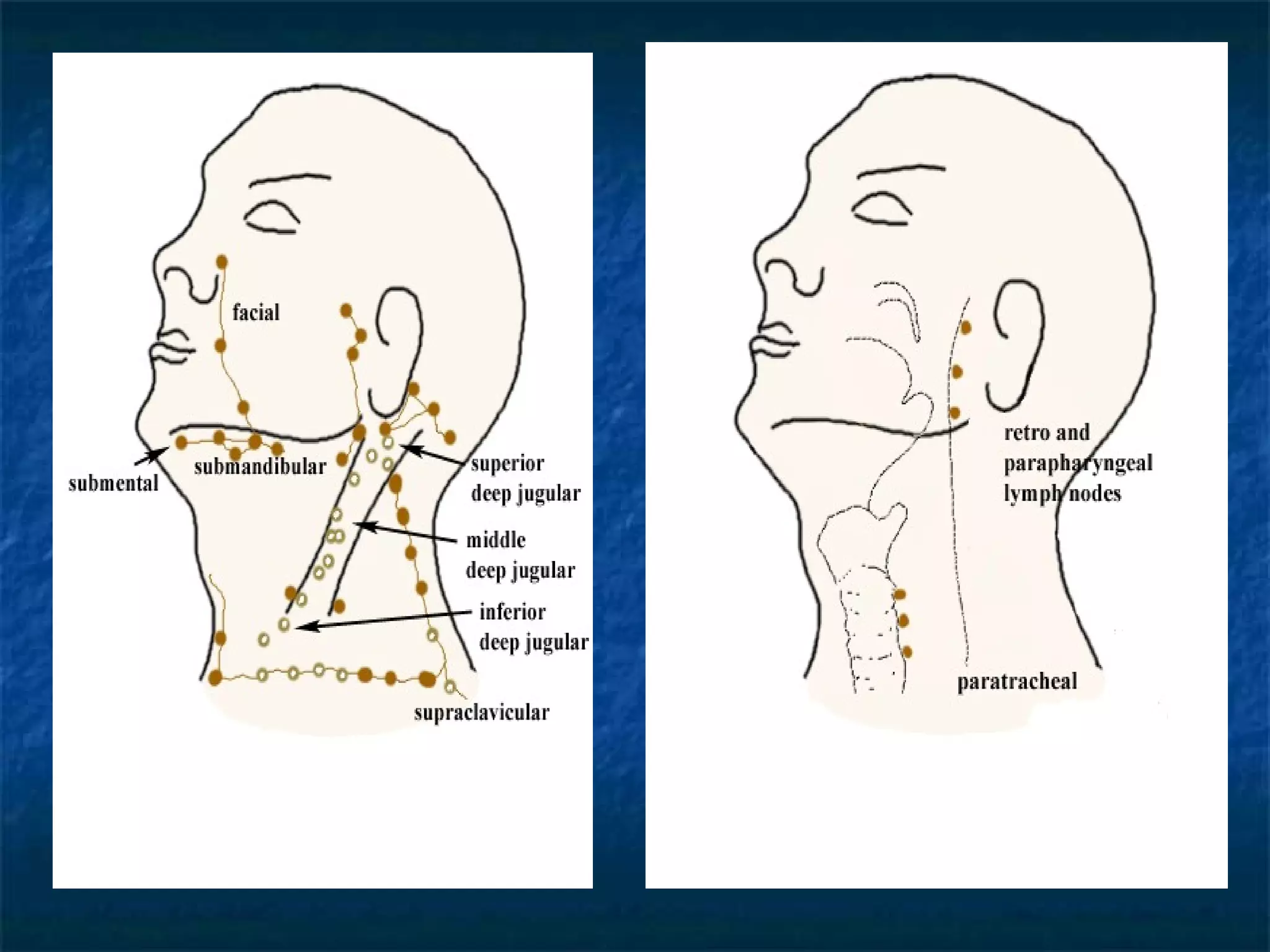
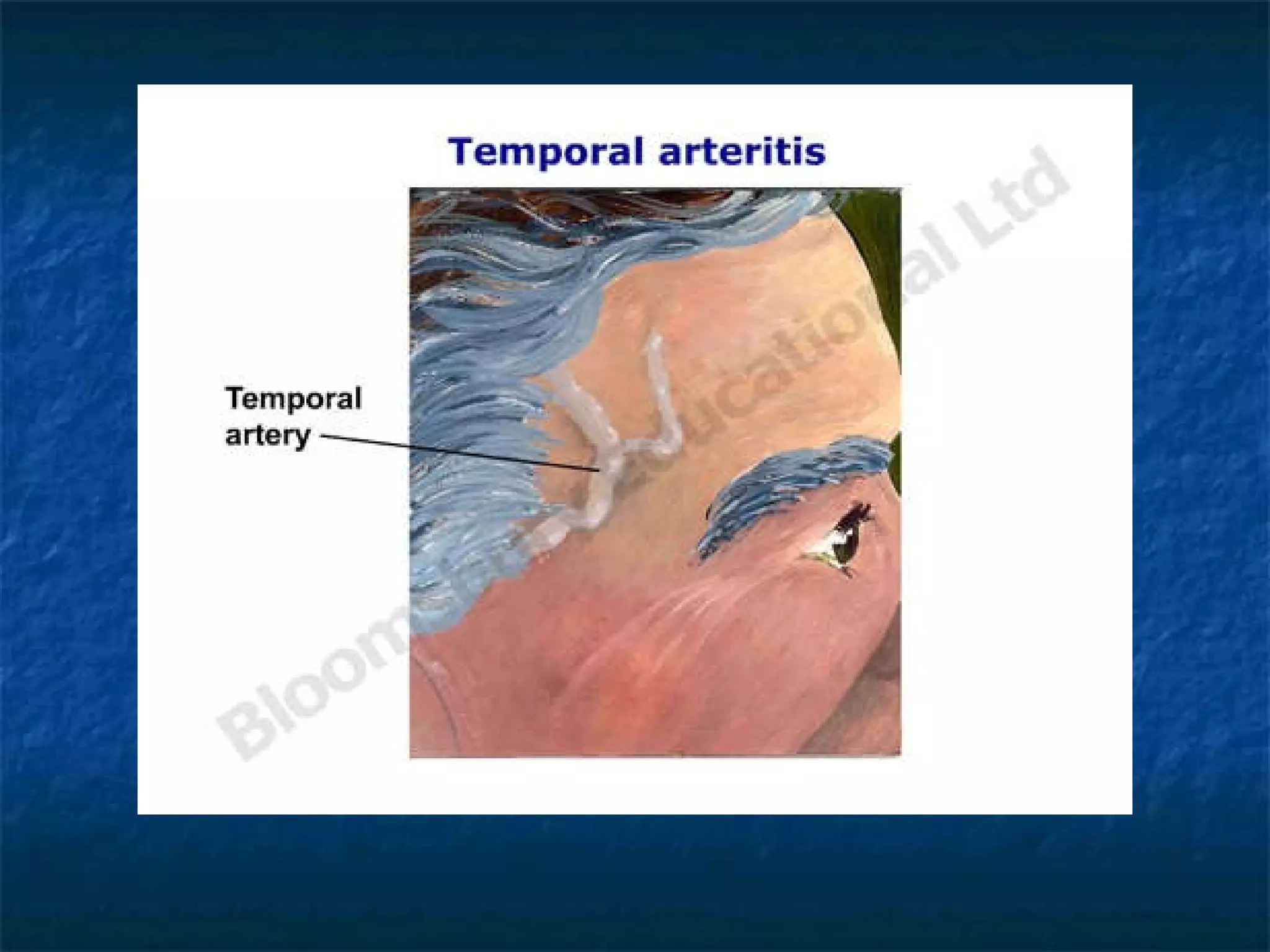
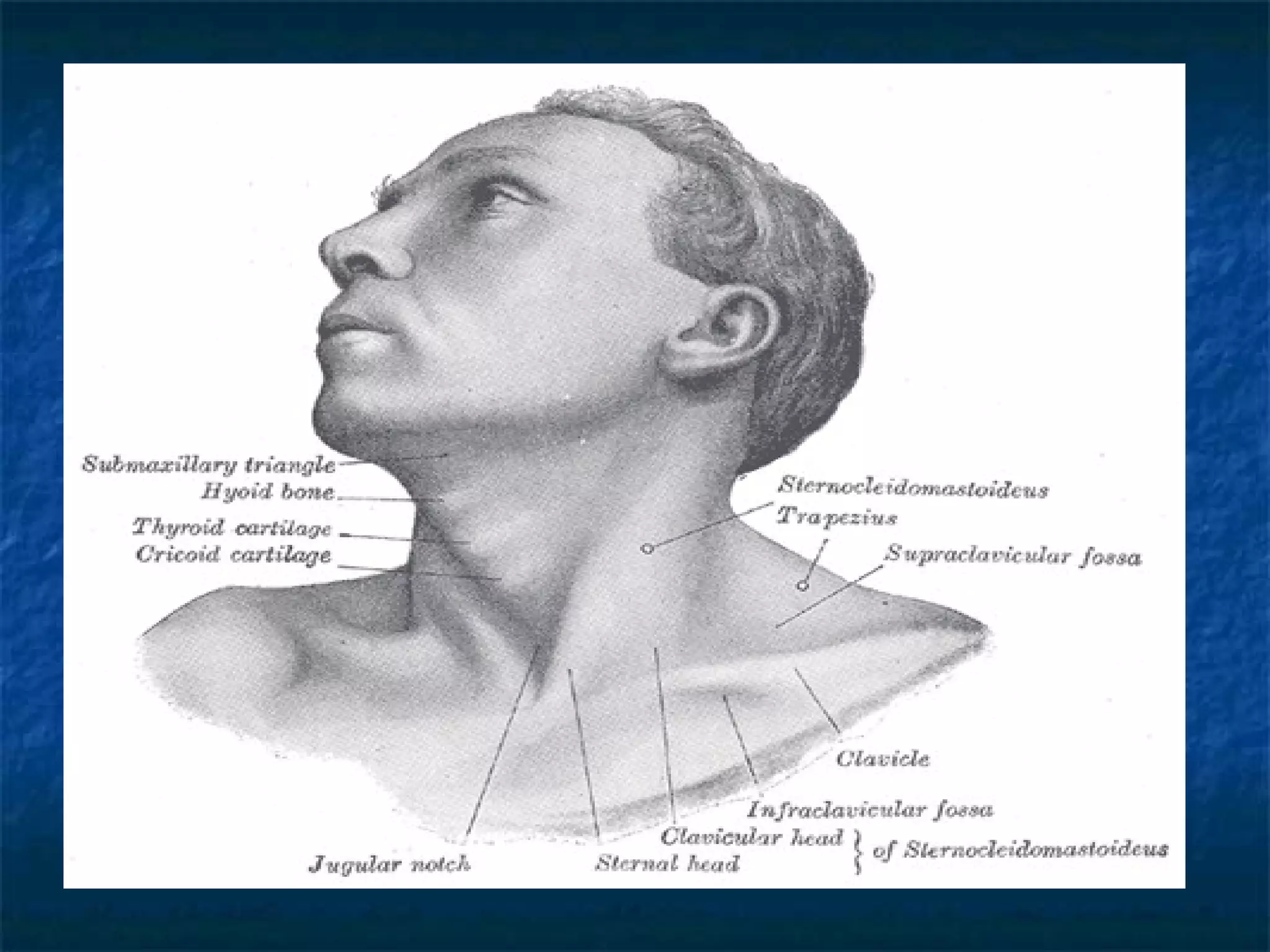
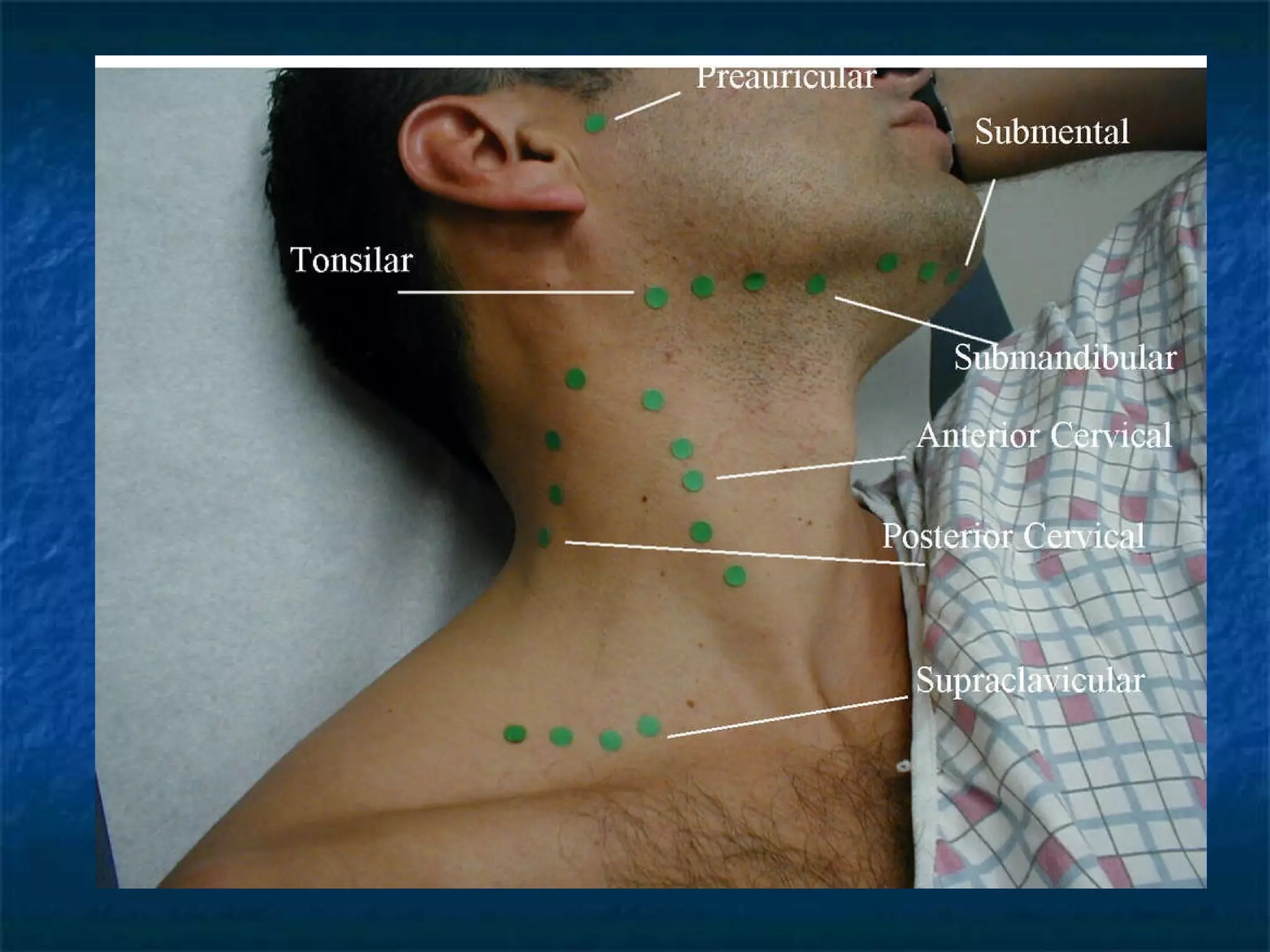
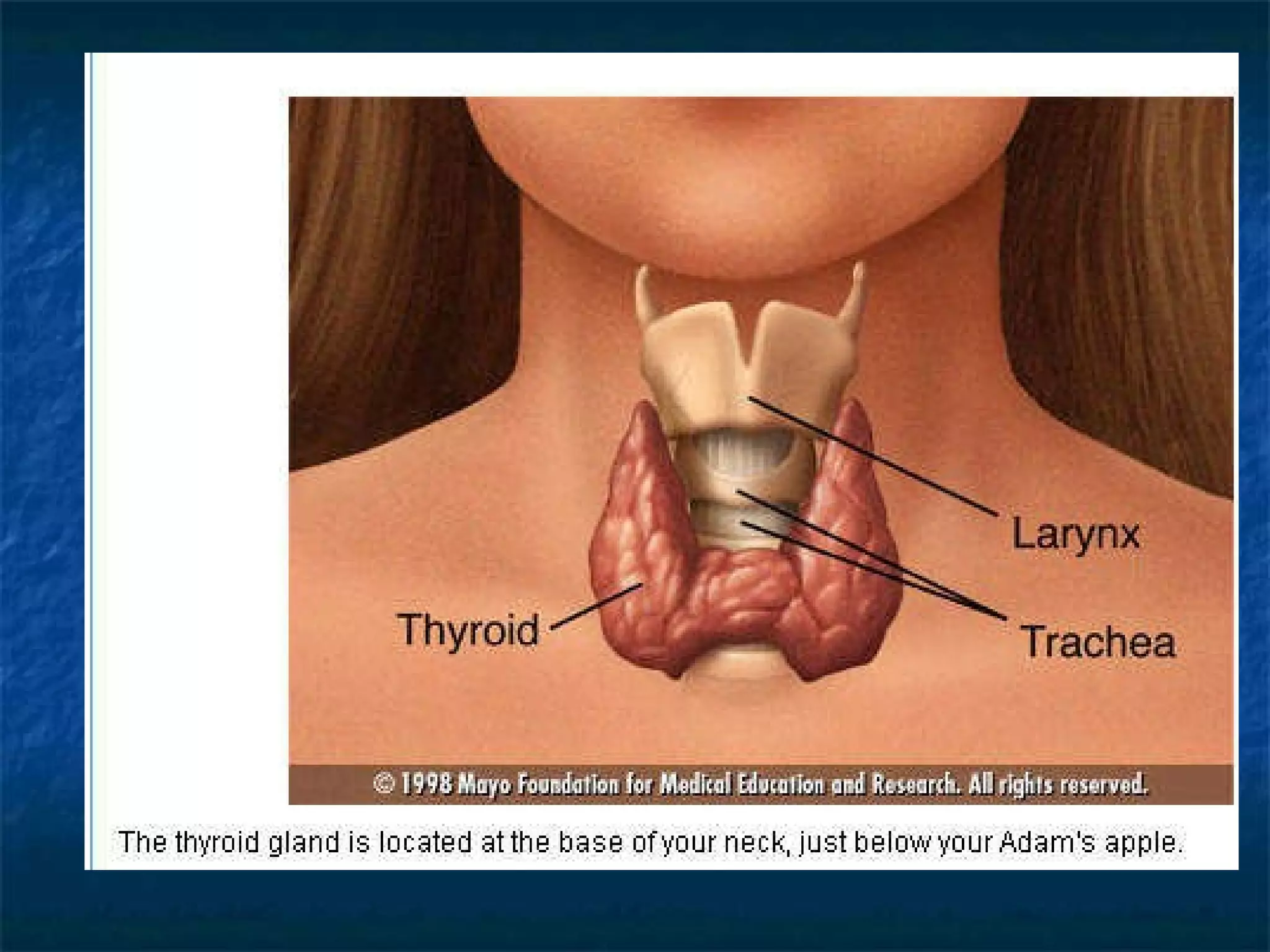
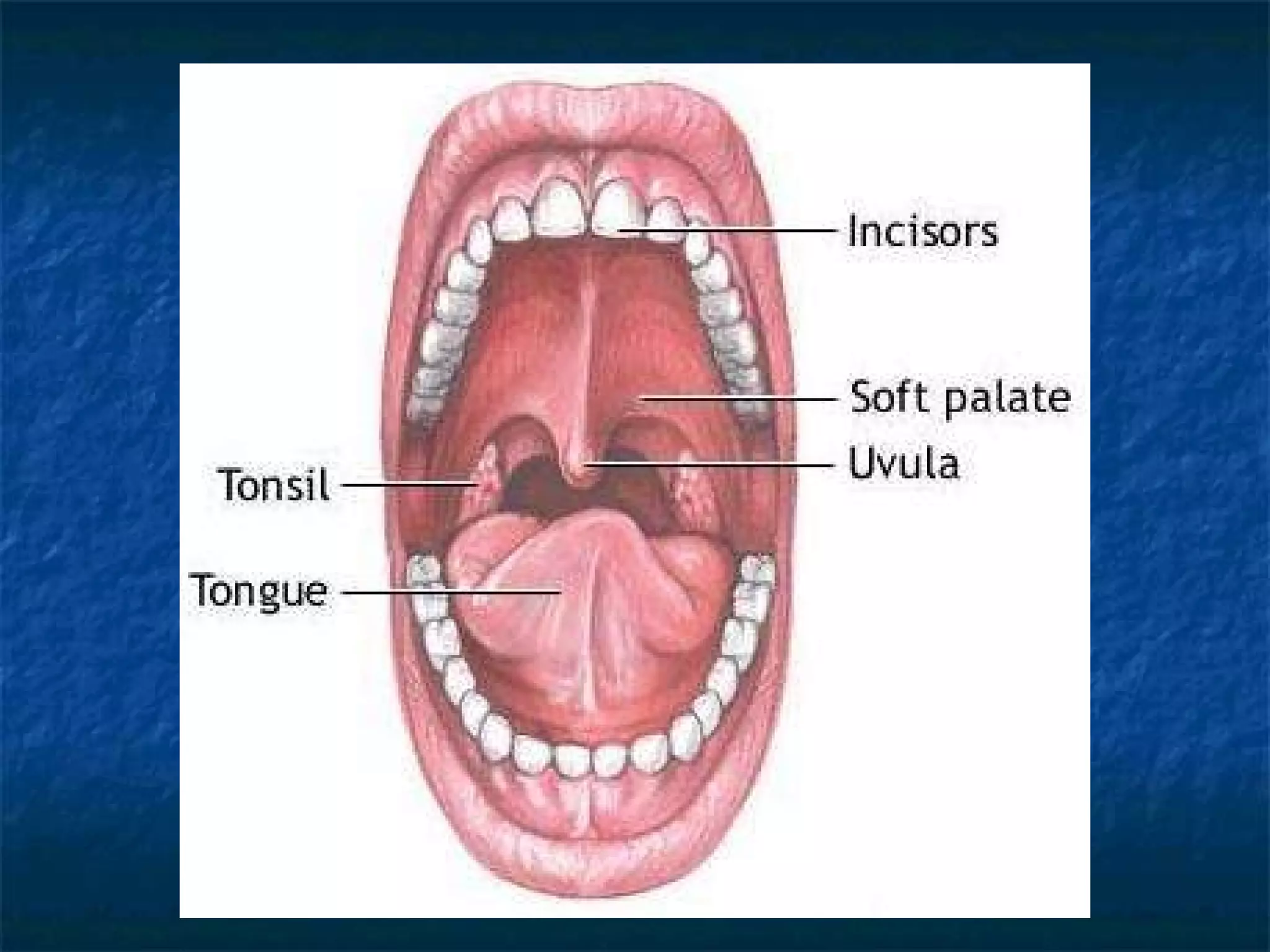
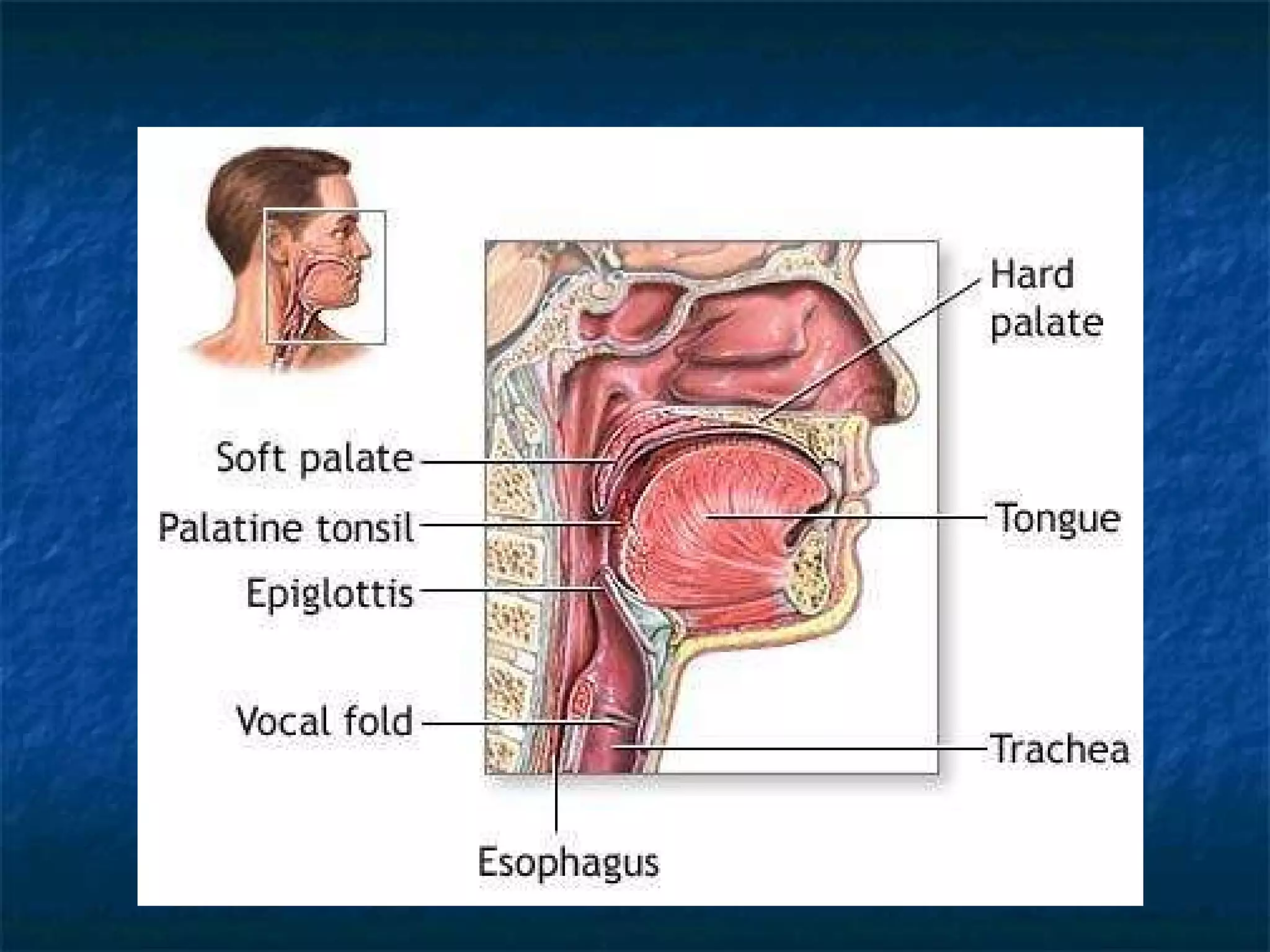
This document provides an overview of conducting a head, eyes, ears, nose, and throat (HEENT) examination. It lists the learning objectives, components to examine, anatomical landmarks, examination procedures, and how to record findings. The key areas covered are inspecting and palpating the head, eyes, ears, nose, mouth, neck, and lymph nodes. Procedures are described for assessing structures like the thyroid, trachea, and temporal arteries. The goal is to identify abnormalities, landmarks, exam techniques, and document examination findings.