Downloaded 1,164 times



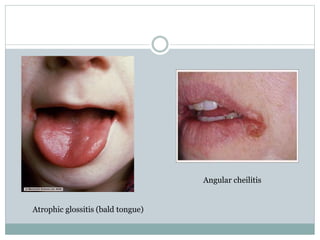


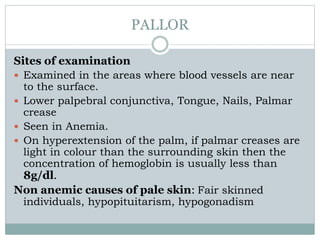







This document provides guidance on assessing nutrition and performing a physical examination. It discusses evaluating body mass index, waist circumference, waist-hip ratio to assess macronutrient status. It also describes clinical signs of various micronutrient deficiencies. Key aspects of the physical exam covered include assessing pallor, icterus, cyanosis, clubbing, lymphadenopathy, and edema. Sites of the body are identified to examine for each of these signs. Common causes associated with abnormal physical findings are also outlined.























































































