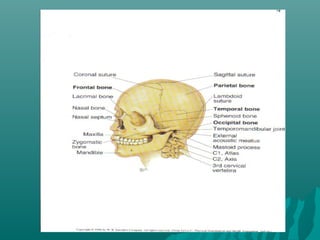
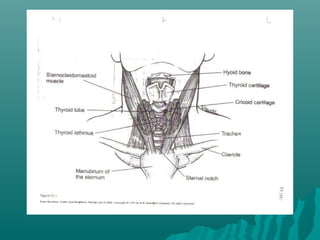
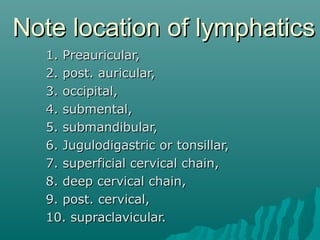
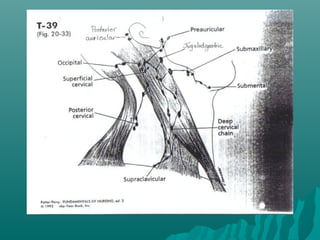
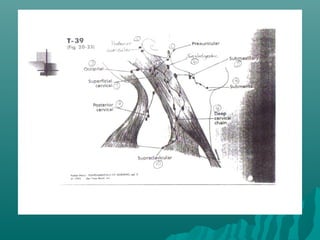
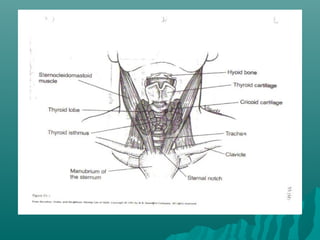
The document provides an overview of the anatomy of the head and neck region, including the bones, muscles, glands, blood vessels and lymphatics. It describes how to inspect, palpate and auscultate each area as part of a physical exam, noting normal findings as well as potential abnormalities. Developmental variations and considerations for different populations are also outlined.