Downloaded 376 times
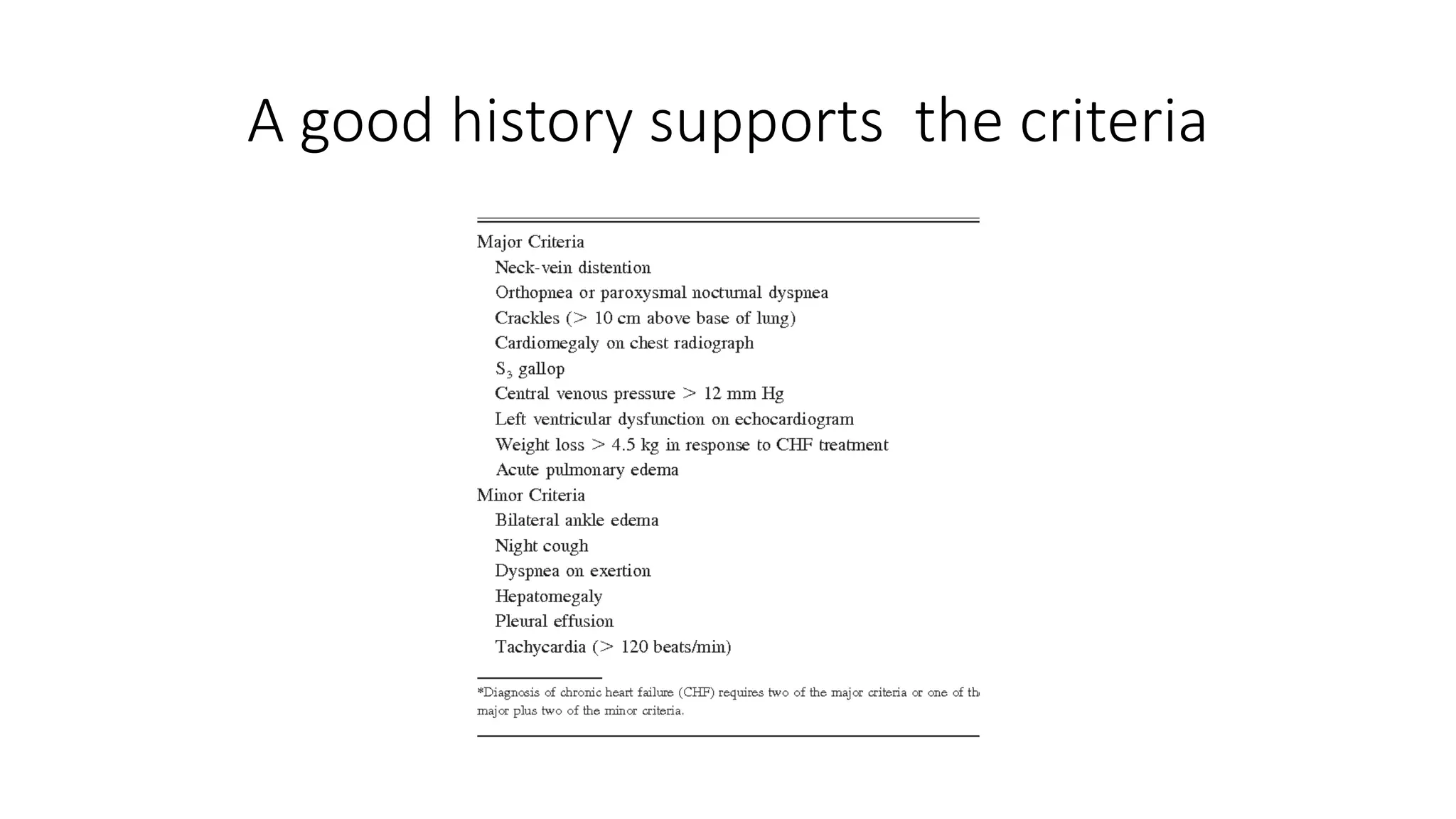















The document outlines a comprehensive guide for taking a cardiovascular patient history without a stethoscope, detailing essential elements such as the presenting complaint, past medical and drug history, family and social history, and systemic enquiry. It emphasizes the importance of asking specific questions related to symptoms, risk factors, and patient context to arrive at a provisional diagnosis. The documentation also highlights the significance of summarizing the information gathered to ensure understanding and accuracy.























































































