Downloaded 472 times

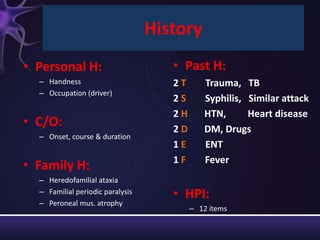

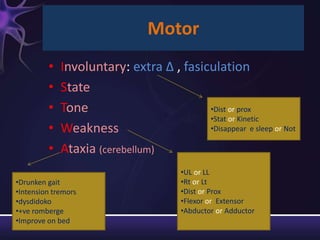
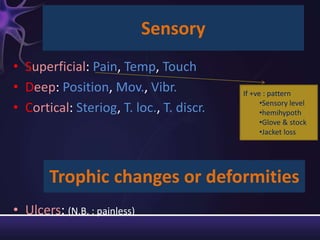
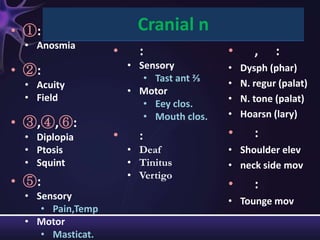
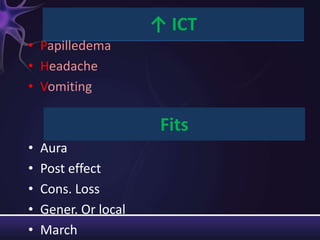
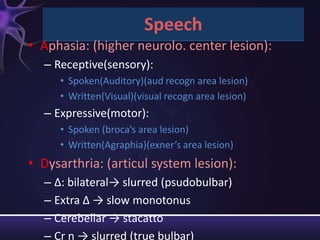
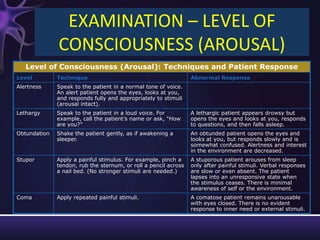
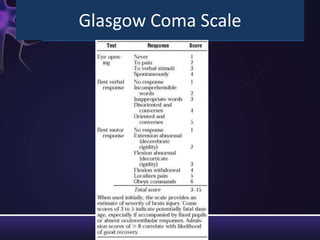
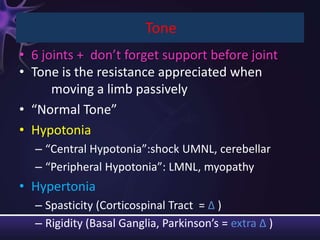
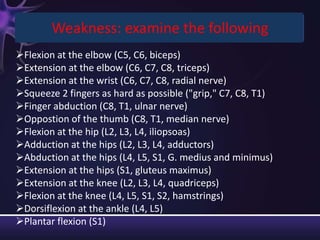
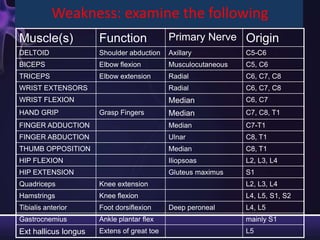

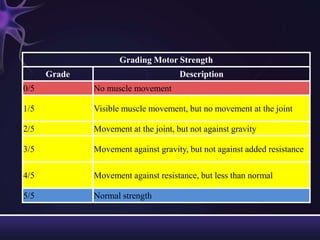
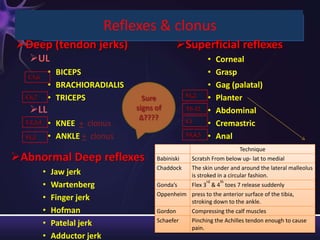
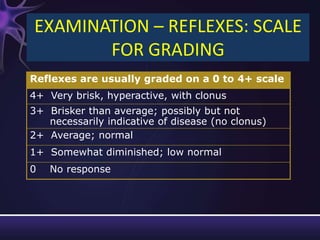
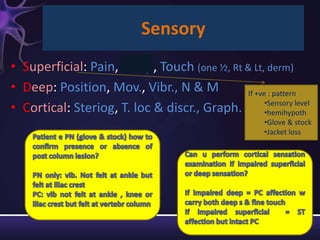
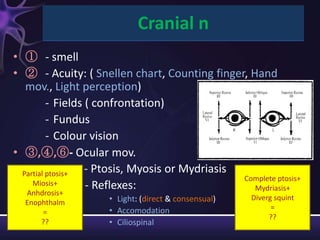
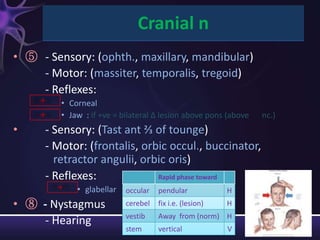
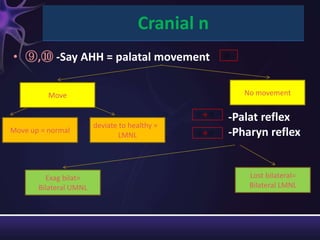


This neurological examination document provides details on: 1) The history, presenting complaints, family history, and review of systems to obtain for a neurological exam. 2) The components of the neurological exam including motor function, sensory function, cranial nerves, reflexes, and mental status. 3) Descriptions of how to examine each system, what abnormalities to look for, and what they may indicate. Rating scales are provided for things like strength, reflexes, and level of consciousness. 4) Common gait patterns and their potential causes are listed at the end.



































































